TWI850139B - Endotracheal tube device - Google Patents
Endotracheal tube deviceDownload PDFInfo
- Publication number
- TWI850139B TWI850139BTW112141709ATW112141709ATWI850139BTW I850139 BTWI850139 BTW I850139BTW 112141709 ATW112141709 ATW 112141709ATW 112141709 ATW112141709 ATW 112141709ATW I850139 BTWI850139 BTW I850139B
- Authority
- TW
- Taiwan
- Prior art keywords
- endotracheal tube
- intubation
- insertion portion
- endotracheal
- aforementioned
- Prior art date
Links
- 238000002627tracheal intubationMethods0.000claimsabstractdescription108
- 238000003780insertionMethods0.000claimsabstractdescription80
- 230000037431insertionEffects0.000claimsabstractdescription80
- 210000004704glottisAnatomy0.000claimsabstractdescription30
- 210000003437tracheaAnatomy0.000claimsabstractdescription24
- 230000008859changeEffects0.000claimsabstractdescription5
- 229910052751metalInorganic materials0.000claimsdescription37
- 239000002184metalSubstances0.000claimsdescription37
- 238000000034methodMethods0.000claimsdescription29
- 230000006870functionEffects0.000claimsdescription16
- 230000005540biological transmissionEffects0.000claimsdescription12
- 229920005989resinPolymers0.000claimsdescription11
- 239000011347resinSubstances0.000claimsdescription11
- YCKRFDGAMUMZLT-UHFFFAOYSA-NFluorine atomChemical compound[F]YCKRFDGAMUMZLT-UHFFFAOYSA-N0.000claimsdescription9
- 229910052731fluorineInorganic materials0.000claimsdescription9
- 239000011737fluorineSubstances0.000claimsdescription9
- 238000005286illuminationMethods0.000claimsdescription8
- 229910001069Ti alloyInorganic materials0.000claimsdescription6
- RTAQQCXQSZGOHL-UHFFFAOYSA-NTitaniumChemical compound[Ti]RTAQQCXQSZGOHL-UHFFFAOYSA-N0.000claimsdescription6
- 239000000463materialSubstances0.000claimsdescription6
- 229920001343polytetrafluoroethylenePolymers0.000claimsdescription6
- 239000004810polytetrafluoroethyleneSubstances0.000claimsdescription6
- 229910001285shape-memory alloyInorganic materials0.000claimsdescription6
- 239000010935stainless steelSubstances0.000claimsdescription6
- 229910001220stainless steelInorganic materials0.000claimsdescription6
- 239000010936titaniumSubstances0.000claimsdescription6
- 229910052719titaniumInorganic materials0.000claimsdescription6
- 229910045601alloyInorganic materials0.000claimsdescription5
- 239000000956alloySubstances0.000claimsdescription5
- 238000010438heat treatmentMethods0.000claimsdescription5
- 238000003384imaging methodMethods0.000claimsdescription5
- 229910001000nickel titaniumInorganic materials0.000claimsdescription4
- 238000012545processingMethods0.000claimsdescription4
- 238000007493shaping processMethods0.000claimsdescription4
- 239000011248coating agentSubstances0.000claimsdescription3
- 238000000576coating methodMethods0.000claimsdescription3
- 239000013307optical fiberSubstances0.000claimsdescription3
- 229920013653perfluoroalkoxyethylenePolymers0.000claimsdescription3
- -1polytetrafluoroethylenePolymers0.000claimsdescription3
- 230000008569processEffects0.000claimsdescription3
- BFKJFAAPBSQJPD-UHFFFAOYSA-NtetrafluoroetheneChemical groupFC(F)=C(F)FBFKJFAAPBSQJPD-UHFFFAOYSA-N0.000claimsdescription3
- 238000004140cleaningMethods0.000abstractdescription12
- 238000009423ventilationMethods0.000description14
- 238000002680cardiopulmonary resuscitationMethods0.000description11
- 230000006378damageEffects0.000description8
- 210000000214mouthAnatomy0.000description8
- 210000000867larynxAnatomy0.000description7
- 230000007547defectEffects0.000description6
- 230000029058respiratory gaseous exchangeEffects0.000description6
- 238000001356surgical procedureMethods0.000description6
- 238000012549trainingMethods0.000description6
- 238000002695general anesthesiaMethods0.000description5
- 210000003800pharynxAnatomy0.000description5
- 238000011282treatmentMethods0.000description5
- 239000004033plasticSubstances0.000description4
- 230000008485antagonismEffects0.000description3
- QVGXLLKOCUKJST-UHFFFAOYSA-Natomic oxygenChemical compound[O]QVGXLLKOCUKJST-UHFFFAOYSA-N0.000description3
- 238000005452bendingMethods0.000description3
- 230000006835compressionEffects0.000description3
- 238000007906compressionMethods0.000description3
- 238000010586diagramMethods0.000description3
- 210000002409epiglottisAnatomy0.000description3
- 210000003238esophagusAnatomy0.000description3
- 210000004072lungAnatomy0.000description3
- 229910052760oxygenInorganic materials0.000description3
- 239000001301oxygenSubstances0.000description3
- 238000004393prognosisMethods0.000description3
- 238000011084recoveryMethods0.000description3
- 206010021143HypoxiaDiseases0.000description2
- 230000003042antagnostic effectEffects0.000description2
- 230000006399behaviorEffects0.000description2
- 230000008901benefitEffects0.000description2
- 239000003814drugSubstances0.000description2
- 239000000835fiberSubstances0.000description2
- 210000003128headAnatomy0.000description2
- 230000006872improvementEffects0.000description2
- 208000015181infectious diseaseDiseases0.000description2
- 238000007689inspectionMethods0.000description2
- 230000014759maintenance of locationEffects0.000description2
- 230000006386memory functionEffects0.000description2
- 239000007769metal materialSubstances0.000description2
- 150000002739metalsChemical class0.000description2
- 238000012797qualificationMethods0.000description2
- 238000007789sealingMethods0.000description2
- 238000004659sterilization and disinfectionMethods0.000description2
- 230000035882stressEffects0.000description2
- 206010002091AnaesthesiaDiseases0.000description1
- 208000002381Brain HypoxiaDiseases0.000description1
- 206010007617Cardio-respiratory arrestDiseases0.000description1
- 208000010496Heart ArrestDiseases0.000description1
- 208000008312Tooth LossDiseases0.000description1
- 230000001154acute effectEffects0.000description1
- 230000032683agingEffects0.000description1
- 230000037005anaesthesiaEffects0.000description1
- 230000003444anaesthetic effectEffects0.000description1
- 229940035676analgesicsDrugs0.000description1
- 239000000730antalgic agentSubstances0.000description1
- 238000002555auscultationMethods0.000description1
- 239000008280bloodSubstances0.000description1
- 210000004369bloodAnatomy0.000description1
- 210000004556brainAnatomy0.000description1
- 230000002612cardiopulmonary effectEffects0.000description1
- 238000012790confirmationMethods0.000description1
- 238000002316cosmetic surgeryMethods0.000description1
- 238000003745diagnosisMethods0.000description1
- 201000010099diseaseDiseases0.000description1
- 208000037265diseases, disorders, signs and symptomsDiseases0.000description1
- 229940079593drugDrugs0.000description1
- 238000005516engineering processMethods0.000description1
- 230000002496gastric effectEffects0.000description1
- 238000002575gastroscopyMethods0.000description1
- 230000036541healthEffects0.000description1
- 230000007954hypoxiaEffects0.000description1
- 230000001146hypoxic effectEffects0.000description1
- 210000000987immune systemAnatomy0.000description1
- 230000009545invasionEffects0.000description1
- 210000001847jawAnatomy0.000description1
- 230000007774longtermEffects0.000description1
- 238000012423maintenanceMethods0.000description1
- 238000004519manufacturing processMethods0.000description1
- 210000002050maxillaAnatomy0.000description1
- 229940035363muscle relaxantsDrugs0.000description1
- 239000003158myorelaxant agentSubstances0.000description1
- 210000003254palateAnatomy0.000description1
- 239000002574poisonSubstances0.000description1
- 231100000614poisonToxicity0.000description1
- 229920001296polysiloxanePolymers0.000description1
- 230000002980postoperative effectEffects0.000description1
- 230000001012protectorEffects0.000description1
- 238000010992refluxMethods0.000description1
- 230000008929regenerationEffects0.000description1
- 238000011069regeneration methodMethods0.000description1
- 230000002040relaxant effectEffects0.000description1
- 229920002050silicone resinPolymers0.000description1
- 239000007787solidSubstances0.000description1
- 230000002269spontaneous effectEffects0.000description1
- 230000001954sterilising effectEffects0.000description1
- 210000002784stomachAnatomy0.000description1
- 210000001519tissueAnatomy0.000description1
- 230000000007visual effectEffects0.000description1
Images
Classifications
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B1/00—Instruments for performing medical examinations of the interior of cavities or tubes of the body by visual or photographical inspection, e.g. endoscopes; Illuminating arrangements therefor
- A61B1/005—Flexible endoscopes
- A61B1/01—Guiding arrangements therefore
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61B—DIAGNOSIS; SURGERY; IDENTIFICATION
- A61B1/00—Instruments for performing medical examinations of the interior of cavities or tubes of the body by visual or photographical inspection, e.g. endoscopes; Illuminating arrangements therefor
- A61B1/267—Instruments for performing medical examinations of the interior of cavities or tubes of the body by visual or photographical inspection, e.g. endoscopes; Illuminating arrangements therefor for the respiratory tract, e.g. laryngoscopes, bronchoscopes
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61M—DEVICES FOR INTRODUCING MEDIA INTO, OR ONTO, THE BODY; DEVICES FOR TRANSDUCING BODY MEDIA OR FOR TAKING MEDIA FROM THE BODY; DEVICES FOR PRODUCING OR ENDING SLEEP OR STUPOR
- A61M16/00—Devices for influencing the respiratory system of patients by gas treatment, e.g. ventilators; Tracheal tubes
- A61M16/04—Tracheal tubes
Landscapes
- Health & Medical Sciences (AREA)
- Life Sciences & Earth Sciences (AREA)
- Surgery (AREA)
- Veterinary Medicine (AREA)
- Pulmonology (AREA)
- Biomedical Technology (AREA)
- Heart & Thoracic Surgery (AREA)
- Public Health (AREA)
- Engineering & Computer Science (AREA)
- Animal Behavior & Ethology (AREA)
- General Health & Medical Sciences (AREA)
- Pathology (AREA)
- Molecular Biology (AREA)
- Physics & Mathematics (AREA)
- Biophysics (AREA)
- Nuclear Medicine, Radiotherapy & Molecular Imaging (AREA)
- Optics & Photonics (AREA)
- Radiology & Medical Imaging (AREA)
- Medical Informatics (AREA)
- Hematology (AREA)
- Anesthesiology (AREA)
- Emergency Medicine (AREA)
- Otolaryngology (AREA)
- Physiology (AREA)
- Endoscopes (AREA)
- Surgical Instruments (AREA)
Abstract
Translated fromChineseDescription
Translated fromChinese本發明係有關於,適合於氣管插管的氣管插管裝置。The present invention relates to an endotracheal intubation device suitable for endotracheal intubation.
在手術等之際,會發生施予全身麻醉的情況。此情況下,被麻醉的患者係因為自主呼吸會被停止,所以必須從外部強制進行換氣,需要擬似性地製造呼吸狀態,並維持之。一般來說,是將一種被稱作氣管內管(氣管內導管)的軟質之樹脂導管從口腔或鼻腔插入,設置於氣管內,透過相反部的口腔外端部而連接至人工呼吸器。During surgery, general anesthesia may be administered. In this case, the patient's spontaneous breathing will be stopped, so ventilation must be forced from the outside, and a simulated breathing state must be created and maintained. Generally, a soft resin tube called an endotracheal tube (endotracheal tube) is inserted from the mouth or nose, placed in the trachea, and connected to a respirator through the outer end of the mouth at the opposite end.
該全身麻醉術中的氣管插管的時間性猶豫,係為麻醉效果展現後的1~2分鐘,必須要在此時間內連接至人工呼吸器。又,不限於上記,事故或疾病等原因而需要緊急連接至人工呼吸器的事態也會經常發生。此情況下也和上記同樣地必須迅速地將氣管插管與人工呼吸器做連接。The time for intubation during general anesthesia is 1 to 2 minutes after the anesthetic effect appears, and the patient must be connected to the artificial respirator within this time. In addition, not limited to the above, there are also frequent situations where an emergency connection to an artificial respirator is required due to accidents or illnesses. In this case, the intubation must be connected to the artificial respirator quickly, just like the above.
氣管插管手技,係為心肺復甦或長期人工呼吸器管理、全身麻醉等中所必須之手技,但在解剖學上的路徑存有個人差異,或因為疾病而會有導致難以插入的情況等等,因此會有若非熟練者或使用昂貴的設備則無法容易進行迅速的氣管插管之情況。Tracheal intubation is a necessary skill for cardiopulmonary resuscitation, long-term artificial respirator management, general anesthesia, etc. However, due to individual differences in anatomical paths and diseases that may make insertion difficult, it may be difficult to perform tracheal intubation quickly without skilled personnel or the use of expensive equipment.
在插管之際,氣管內管係通過口腔、咽頭及聲門而被插入設置至氣管內。作為插管有被確實進行的狀態,係為在口腔、咽頭、喉頭的軸為一致的直線上能夠觀察到聲門為理想,但就通常的縱臥位而言在解剖學上來說軸不會一致,因此是從一種被稱作嗅吸姿勢(Sniffing position)的使用到墊枕的類似就寢體位之狀態起,讓頭頂部往肩側反折,以使軸呈現一致。During intubation, the endotracheal tube is inserted into the trachea through the oral cavity, pharynx, and glottis. Ideally, the glottis can be observed on a straight line with the axis of the oral cavity, pharynx, and larynx aligned, but the axis is not aligned anatomically in the normal longitudinal lying position, so the axis is aligned by using a sniffing position or a pillow-like sleeping position, with the top of the head folded back toward the shoulder.
即使在此狀態下觀察咽頭,也會被會厭的背面所遮擋,而無法看見聲門。因此,在實際的觀察時,係使用一種被稱作喉頭鏡的器具把葉柄的尖端抵接於會厭谷,使會厭間接地抬起,試圖撐開喉頭,以確認聲門(例如參照專利文獻1)。Even if the pharynx is observed in this state, the back of the epiglottis will block the glottis. Therefore, in actual observation, an instrument called a laryngoscope is used to place the tip of the petiole against the epiglottis, so that the epiglottis is indirectly lifted and the larynx is pushed open to confirm the glottis (see, for example, Patent Document 1).
經由該程序後,將一種稱作通條的治具插入氣管內管,對通條的尖端側賦予任意之彎曲後,把喉頭鏡葉柄當作導軌同時把氣管內管逐漸送進聲門內。突破聲門後,將通條從氣管內管拔出,推送氣管內管,完成插管。其後,裝上人工呼吸用的甦醒球並進行送氣,以聽診確認沒有發生食道插管或只對單肺換氣。After this procedure, a tool called a cleaning rod is inserted into the endotracheal tube. After the tip of the cleaning rod is bent to any angle, the endotracheal tube is gradually pushed into the glottis using the laryngoscope handle as a guide. After breaking through the glottis, the cleaning rod is pulled out of the endotracheal tube, and the endotracheal tube is pushed in to complete the intubation. Afterwards, a resuscitation ball for artificial respiration is installed and air is supplied, and auscultation is performed to confirm that no esophageal intubation or ventilation of only one lung has occurred.
然後,使用針筒將所定之空氣量打入氣管內管的氣球而使其膨脹,藉此以防止逆流等。最後為了防止氣管內管之破損,用咬塊讓患者咬住,將兩者使用專用的膠帶加以固定後,在患者的口角將氣管內管使用專用的膠帶加以固定。Then, a predetermined amount of air is pumped into the balloon of the endotracheal tube using a syringe to inflate it, thereby preventing backflow, etc. Finally, in order to prevent damage to the endotracheal tube, a bite block is used for the patient to bite, and the two are fixed with special tape, and the endotracheal tube is fixed with special tape at the corner of the patient's mouth.
如此的手技係要求迅速性與精密性,先前以來有各式各樣的專用治具/機器已被提出且實用化。一般經常被使用的一例也就是視訊喉頭鏡(例如參照專利文獻2),係在喉頭鏡的尖端安裝有CCD攝影機,可不須直接目視就能觀察咽頭的撐開狀態,已經有各式各樣的機種被販售、普及,但視野只到咽頭部為止,聲門通過後的食道誤插管等之事象係難以瞬時判斷,有此缺點。又,硬質喉頭鏡係由於是使硬質葉柄接觸於牙齒而使用的形態,因此隨著患者的牙齒的狀態或缺損狀態而可能會造成損傷等,會有難以使用的情況。Such manual techniques require speed and precision, and various special jigs/machines have been proposed and put into practical use. A commonly used example is a video laryngoscope (for example, refer to Patent Document 2), which has a CCD camera installed at the tip of the laryngoscope, and can observe the stretched state of the pharynx without direct visual observation. Various models have been sold and popularized, but the field of view only reaches the pharynx, and it is difficult to instantly judge the phenomenon of esophageal intubation after the glottis passes, which has this disadvantage. In addition, since the hard laryngoscope is used in a form that makes the hard petiole contact the teeth, it may cause damage to the patient's teeth depending on the state or defect of the teeth, which may make it difficult to use.
另1個例子係為,一種被稱作光纖內視鏡的內視鏡型之機器(例如參照專利文獻3)。雖然可以插入氣管內管內,觀察到聲門通過後的患部,但並無像是通條般的形狀記憶性,必須以和內視鏡同等之操作而一面維持形狀一面施術,施術者的熟練性係被要求,而有無法泛用的缺點。無論如何,既有的機器係為昂貴,難以在有需要的醫療現場或救急設備上普遍地裝備,存有此一問題。Another example is an endoscope-type device called a fiber endoscope (see, for example, Patent Document 3). Although it can be inserted into the endotracheal tube to observe the affected area after passing through the glottis, it does not have the shape memory like a cleansing rod, and the operation must be performed while maintaining the shape in the same way as an endoscope. The proficiency of the operator is required, and there is a disadvantage that it cannot be widely used. In any case, the existing device is expensive and it is difficult to be widely equipped in medical sites or emergency facilities where it is needed.
[既有技術所存在的問題] 氣管插管手技係與生命直接關連,施術的容易化與安全性的提升係被強烈要求。根據此一背景而過去已經有各式各樣的技法或治具被開發且改善,但就算到了現代,最能劃分手技之成否的因素,仍是受到事前的資訊確認與術者的技能、經驗值所影響。雖然已經有各式各樣的治具機器被研發並活用,但相較於用途的重大性,效用的範圍是受到限定的,綜合來說,能夠提升手技的效率或安全性的設備係不存在。[Problems with existing technologies]Tracheal intubation techniques are directly related to life, and there is a strong demand for easier and safer procedures. Based on this background, various techniques and jigs have been developed and improved in the past, but even in modern times, the most important factor that determines the success of techniques is still the prior information confirmation and the skills and experience of the operator. Although various jigs and machines have been developed and used, the scope of their effectiveness is limited compared to the importance of their uses. Generally speaking, there is no equipment that can improve the efficiency or safety of techniques.
例如,硬性喉頭鏡係由於具備視訊攝影機和螢幕因而容易確認聲門部,可提高插管開始時的視認性,但聲門部通過後的內視鏡的確認係為不可能,無法防止誤插管等。軟性內視鏡,係可因應需要而使特定的部位做變形,且插管困難時的患部確認也為可能,但是施術上需要熟練的操作技術。For example, a rigid laryngoscope is equipped with a video camera and a screen, so it is easy to check the glottis, which can improve visibility at the beginning of intubation, but it is impossible to check the glottis with an endoscope, and it cannot prevent wrong intubation, etc. A flexible endoscope can be deformed to a specific part as needed, and it is also possible to check the affected part when intubation is difficult, but the operation requires skilled operation skills.
所述之手技造成的意外或事故雖然推測難以呈現在醫療統計等上,但若也考慮到需要所述之手技的情況下熟練者並不一定在場的事案,也可想而知有可能以一定的頻率發生悲劇。從臨床醫療的現場來看,凌駕既有的機器,且操作容易不需要精通的安全且簡潔的氣管插管手技治具的出現,是被人們所期望。Although it is difficult to predict the accidents or incidents caused by the above-mentioned technique in medical statistics, if we also consider that the skilled person may not be present when the above-mentioned technique is required, it is conceivable that tragedies may occur with a certain frequency. From the perspective of clinical medicine, the emergence of a safe and simple tracheal intubation technique jig that overrides existing machines and is easy to operate without requiring proficiency is expected.
作為醫院內的醫療行為,護理師的氣管插管手技之是非,長年以來一直為人所議論。基本上在外科醫院內的氣管插管行為,係以需要全身麻醉的手術為目的居多,基本上是有測定計畫並有準備的行為。有被預定並準備的氣管插管行為主要是與麻醉藥併用鎮痛劑或肌肉鬆弛劑等,是意識到患者的狀態管理與術後的回復等而被進行。As a medical practice in hospitals, the pros and cons of nurses' tracheal intubation skills have been a topic of debate for many years. In general, tracheal intubation in surgical hospitals is mostly for the purpose of surgery that requires general anesthesia, and is basically a planned and prepared practice. Intubation that is planned and prepared is mainly performed with anesthesia and analgesics or muscle relaxants, and is performed with the patient's condition management and postoperative recovery in mind.
該行為係需要非常專門的知識和技術,因此關於插管/拔管皆同樣地會被慎重考慮。又,即使是身為有資格者的醫師,實際情況下這也並非所有的醫師都能有自信地實施的手技,擁有扎實實技技能者通常是麻醉科醫師和急診室醫師等,會有某種程度受到限定的傾向。This behavior requires very specialized knowledge and skills, so intubation/extubation are also carefully considered. In addition, even if they are qualified doctors, in reality, not all doctors can confidently perform this skill. Those who have solid practical skills are usually anesthesiologists and emergency room doctors, so there is a tendency to be limited to a certain extent.
因此,雖然是物理上侵入程度較低的醫療行為,但手技的速度和精度直接關連到生死,而且也會對預後帶來影響,因此護理師的氣管插管手技被判斷為並非理想的情況為多。插管行為,係除了緊急復甦時以外,應該是被縝密地計畫並管理才被允許進行的手技。在醫院內的醫療行為中就算是有十二分把握實技技能的麻醉科醫師,也並非對現狀的氣管插管手技治具保持滿足並完全放心地信賴,許多醫師也期望能有更確實且資訊量更多且安全度與迅速性更優異的氣管插管手技治具之出現。Therefore, although it is a medical procedure with a low degree of physical invasion, the speed and accuracy of the technique are directly related to life and death, and will also affect the prognosis. Therefore, the tracheal intubation technique of nurses is often judged to be not ideal. Intubation is a technique that should be carefully planned and managed before it is allowed, except during emergency resuscitation. In the medical practice in the hospital, even anesthesiologists who have a full grasp of the actual skills are not satisfied with the current tracheal intubation technique jigs and trust them completely. Many doctors also hope that there will be more accurate and more informative tracheal intubation technique jigs with better safety and speed.
在急救救命的現場中,先前係由於氣管插管手技的專門性,因此伴隨著氣管插管的換氣係限定為醫師,但現在由於對救命率的提升與搬送時的樣態之改善/維持產生了期待,因此已經被認為是「僅在醫師所致之實施為不可能的醫院前救護中心肺機能停止狀態此一限定狀況下可能的復甦行為」,自2004年7月起「以事前及事後的醫療控管體制之完備為條件,經過一定之講習及醫院實習結業,而受到認證的緊急救護技術員」已被正式認可能夠進行之。In the field of emergency rescue, ventilation accompanying tracheal intubation was previously limited to physicians due to the specialized nature of tracheal intubation techniques. However, now that there is an expectation for an increase in the life-saving rate and an improvement/maintenance of the state during transportation, it has been recognized as "a possible resuscitation behavior under the limited condition of pre-hospital emergency cardiopulmonary arrest, which is impossible for physicians to perform." Since July 2004, "emergency rescue technicians who have completed certain training and hospital internships and have been certified, with the establishment of a pre- and post-hospital medical control system, have been officially recognized as being able to perform it."
醫師不在場的非熟練者之手技實施雖然單肺插管或食道插管等之瑕疵發生等的頻率會變高,但作為緊急的復甦行為是非常地有用。緊急復甦行為中的插管手技之限制放寬係拉高了復甦救命率,但於急救救命之現場中也是,凌駕既有的機器,且操作容易不需要精通的安全且簡潔的氣管插管手技治具的出現,是被人們所期望。Although the frequency of defects such as single-lung intubation and esophageal intubation will increase when the inexperienced person performs the technique without the presence of a doctor, it is very useful as an emergency resuscitation. Relaxing the restrictions on intubation techniques in emergency resuscitation will increase the recovery and life-saving rate, but in the scene of emergency life-saving, the emergence of a safe and simple tracheal intubation technique jig that can override existing machines and is easy to operate without requiring proficiency is also desired.
部分的救命急救車輛已經裝備有人工呼吸器或氣管插管用具,而已經成為能夠讓受到認證的緊急救護技術員執行氣管插管行為的體制,但特別是既有的視訊喉頭鏡等由於價格昂貴而無法普遍地配備,實際上看不到急速的普及。急救現場中的插管想定會是非常困難的情況,就算是由麻醉科醫來進行,推測插管困難的病例仍不會少。Some emergency vehicles are equipped with artificial respirators or tracheal intubation equipment, and a system has been established that allows certified emergency medical technicians to perform tracheal intubation. However, the existing video laryngoscopes are expensive and cannot be widely equipped, and there is no rapid popularization. Intubation at the emergency scene is bound to be a very difficult situation. Even if it is performed by an anesthesiologist, there are still many cases where intubation is difficult.
許多場合,在如此的狀況下的插管手技,與其使用(直視型)喉頭鏡不如使用視訊喉頭鏡反而被認為較容易且迅速,但現實上(直視型)喉頭鏡已經成為緊急救護技術員的認證規格品,反倒是視訊喉頭鏡的使用上需要追加的講習與實習。該事例推測也是由於視訊喉頭鏡的價格過度地昂貴而無法普遍地配備所造成,這就表示,除了設備的機能提升以外,價格也需要充分地降低。In many cases, intubation techniques in such situations are considered easier and faster with a video laryngoscope than with a (direct view) laryngoscope. However, in reality, the (direct view) laryngoscope has become a certified product for emergency medical technicians, while the use of the video laryngoscope requires additional training and practice. This is probably because the price of the video laryngoscope is too expensive and cannot be widely equipped. This means that in addition to improving the function of the equipment, the price also needs to be sufficiently reduced.
在緊急救護技術員的插管資格認證中,係除了使用假人的訓練以外,也會在有醫師見證且經患者同意後進行實習訓練,但在多數情況下在資格取得後就沒有頻繁進行手技的機會,因此熟習度的持續係為困難。就這點來看也是,凌駕既有的機器,且操作容易不需要精通的安全且簡潔的氣管插管手技治具的出現,是被人們所期望,且其利用的認可也是被人們所期望。In the intubation qualification certification of emergency medical technicians, in addition to training using dummies, practical training is also conducted with the witness of a doctor and the consent of the patient. However, in most cases, there is no opportunity to frequently practice manual skills after obtaining the qualification, so it is difficult to maintain proficiency. In this regard, the emergence of a safe and simple tracheal intubation manual skill jig that overrides existing machines and is easy to operate and does not require proficiency is expected, and its use is also expected to be recognized.
於民眾的急救救命(心肺復甦=CPR)現場中,不使用器具或醫藥品即進行的一次救命處置(Basic Life Support;BLS),胸骨壓迫係為基本,氣道確保或嘴對嘴所致之換氣輔助係被認為是「救助者有受過人工呼吸之訓練,且有進行其之技術與意思的情況」。醫師或緊急救護技術員到場,在BLS沒有效果的情況下所進行的氣管插管或氧氣吸入/人工呼吸器連接等係被分類成二次救命處置(Advanced Life Support;ALS),但在現代的都市部中,自動體外心臟電擊去顫器(AED)係已經普及,在BLS的階段中民眾嘗試進行AED的案例也日益增加。In the first aid (cardiopulmonary resuscitation = CPR) scene of the public, the primary life-saving treatment (Basic Life Support; BLS) is performed without the use of equipment or medicines. The sternal compression is the basic, and airway assurance or mouth-to-mouth ventilation assistance is considered to be "the rescuer has received artificial respiration training and has the skills and intention to perform it." When doctors or emergency medical technicians arrive at the scene, tracheal intubation or oxygen inhalation/artificial respirator connection are performed when BLS is ineffective. These are classified as secondary life-saving treatments (Advanced Life Support; ALS). However, in modern urban areas, automated external defibrillators (AEDs) have become popular, and the number of cases where people try to use AEDs during the BLS stage is increasing.
人類的腦經常需要氧氣,呼吸停止起4~6分鐘左右就會陷入致命性的低氧狀況。一般來說2分鐘以內開始心肺復甦的情況下的救命率係為90%左右,但在4分鐘時就降到50%,在5分鐘時就降到25%左右。氣道確保或嘴對嘴所致之換氣實施不但需要訓練而且長時間的換氣持續係為困難。又,在直接面對現實中場面的情況下,由於感染症的疑慮或毒物等所致之罹災疑慮及施術形態的心理抗拒感,CPR被認為會有猶豫的傾向,因此原本有用的換氣之實施,也會有被降低努力義務的一面。The human brain constantly needs oxygen, and the person will fall into a fatal hypoxic state about 4 to 6 minutes after breathing stops. Generally speaking, the life-saving rate is about 90% when cardiopulmonary resuscitation is started within 2 minutes, but it drops to 50% at 4 minutes and to about 25% at 5 minutes. Airway securing or mouth-to-mouth ventilation not only requires training, but it is also difficult to continue ventilation for a long time. In addition, when facing real-life scenes, CPR is believed to be hesitant due to concerns about infection or disasters caused by poisons, etc., and psychological resistance to the form of the operation, so the implementation of ventilation, which is originally useful, will also be reduced.
民眾所做的插管行為之是非是需要慎重議論的事象,但超出BLS之定義範疇的AED都已經被活用時,未進行有效的換氣行為對策,也被認為是一種不公平。尤其是在災害發生時或大規模事故之發生時或是在郊外地區、離島地區等,想定民眾的CPR行為時間與搬送時間會變長,至少併用自己膨脹式復甦甦醒球(袋瓣罩甦醒球)等所致之手動換氣,想定是較為理想的。最好還是基於醫師之指示而由受過訓練的民眾來進行插管換氣,這可說是最佳的換氣實施方案。無換氣導致缺氧而結果導致的復甦困難可被改善,對於救命後因腦缺氧而結果導致的後遺症展現之低減,也被認為是有用的。這件事情的實現上,凌駕既有的機器,且操作容易不需要精通的安全且簡潔的氣管插管手技治具的出現,係為不可或缺。The right and wrong of intubation by the public is a matter that needs to be carefully discussed, but when AEDs beyond the definition of BLS are already in use, it is also considered unfair not to take effective ventilation measures. Especially in the event of a disaster or a large-scale accident or in rural areas or offshore islands, it is assumed that the CPR time and transportation time of the public will be longer, and it is assumed that manual ventilation using a self-inflating resuscitation ball (bag-valve mask resuscitation ball) is more ideal. It is best to have trained citizens perform intubation and ventilation based on the doctor's instructions, which can be said to be the best ventilation implementation plan. The difficulty in resuscitation caused by hypoxia due to lack of ventilation can be improved, and it is also considered to be useful for reducing the sequelae caused by brain hypoxia after life-saving. In order to achieve this, the emergence of a safe and simple tracheal intubation manual tool that can override existing machines and is easy to operate without requiring proficiency is indispensable.
使用硬性喉頭鏡的施術中牙齒的破損或脫臼、口腔內損傷等之傷害發生,會以一定的頻繁度而發生。在硬性喉頭鏡的使用中,由於硬質葉柄是接觸於上顎前齒並作為支點才能作用,存有結構上、物理上的缺點,就算是健康的牙齒狀態,也可能受到過大的荷重而導致發生脫臼或亞脫臼、或發生破損等等,無法排除這些風險。During the use of a rigid laryngoscope, injuries such as tooth breakage or dislocation, and oral injuries occur with a certain frequency. During the use of a rigid laryngoscope, since the hard petiole is in contact with the front teeth of the upper jaw and acts as a fulcrum, there are structural and physical defects. Even if the teeth are healthy, they may be subjected to excessive loads and cause dislocation or subdislocation, or damage, etc. These risks cannot be eliminated.
有別於此,在現代需要全身麻醉等,在該手術不伴隨緊急性的情況,則事前可準備性地接受牙科的檢查與治療,可謀求術中以及預後的感染症/併發症之減少。在手術的迅速性為優先的情況,則可作成一種被稱作牙套的個人專用之咬嘴並裝著,或可換成操作難易度高的使用軟性喉頭鏡的插管手技。若考慮術後的免疫力低落則改善牙齒或口腔狀態是較為合適的,但是改善或治療需要花費時間,且牙套製作上也會有無法達到即時性的情況。In contrast, in modern times, general anesthesia is required. If the surgery is not accompanied by acute complications, dental examinations and treatments can be performed in advance to reduce the risk of infection and complications during and after the surgery. If the speed of the surgery is a priority, a mouthpiece called a mouthpiece can be made and worn, or a flexible laryngoscope can be used for intubation, which is difficult to operate. If the immune system is weakened after the surgery, it is more appropriate to improve the condition of the teeth or mouth, but improvement or treatment takes time, and the production of the mouthpiece may not be immediate.
作為次佳的解決方案,作為氣管插管用的前齒保護器已經上市,但其係基於一般的成人之牙齒構成而設計,並不一定能夠泛用性地適用,存有如此缺點。 [先前技術文獻] [專利文獻]As a second-best solution, front teeth protectors for tracheal intubation have been marketed, but they are designed based on the structure of general adult teeth and are not necessarily universally applicable, thus having such a shortcoming.[Prior technical literature][Patent literature]
[專利文獻1]日本特開2022-093553號公報 [專利文獻2]日本特開2015-166019號公報 [專利文獻3]日本特開2003-033318號公報[Patent Document 1] Japanese Patent Publication No. 2022-093553[Patent Document 2] Japanese Patent Publication No. 2015-166019[Patent Document 3] Japanese Patent Publication No. 2003-033318
[發明所欲解決之課題][The problem that the invention wants to solve]
如上述,使用到硬性喉頭鏡(例如參照專利文獻1)的氣管插管係在聲門通過後無法做視覺性確認,因此無法防止單肺插管或食道插管等之致命性事故。另一方面,可被視為與氣管插管同等之經口插管行為的胃等之內視鏡觀察,係在一般的定期健康診斷中被常用到認為是安全的檢查行為。在所謂的胃攝影機之診療中,首先不可能有往氣管的誤插管事例,該差異係由於聲門通過後之內視是否為可能,可以說是產生了極端的安全性之差異。以此為用途的作為軟性喉頭鏡的光纖內視鏡產品雖然存在(例如參照專利文獻2),但非常地昂貴,而且操作上要求高度的技術,因此被限定使用於被預想為特別困難的病例上。As mentioned above, tracheal intubation using a rigid laryngoscope (e.g., see Patent Document 1) cannot be visually confirmed after the glottis is passed, and therefore cannot prevent fatal accidents such as single-lung intubation or esophageal intubation. On the other hand, endoscopic observation of the stomach, etc., which can be considered as an oral intubation equivalent to tracheal intubation, is a commonly used and safe examination in general regular health examinations. In the diagnosis of so-called gastroscopy, first of all, there is no possibility of mistaken intubation into the trachea. This difference is due to whether internal observation after the glottis is passed, which can be said to have an extreme difference in safety. Although there are fiber optic endoscope products that are flexible laryngoscopes for this purpose (for example, see Patent Document 2), they are very expensive and require advanced skills to operate, so their use is limited to cases that are expected to be particularly difficult.
無論如何,硬性喉頭鏡係因為硬性葉柄而有傷及牙齒或唇、舌、口腔內的風險,而且就連上顎前突也必須要慎重應對,存有如此缺點。越是不熟練的人,在將固定彎曲的葉柄插入之際,心理上越容易產生誤解而越強力把頭部往後掰屈,此情況下會有容易導致頸椎的損傷、或牙齒的損傷之傾向。甚至在前齒已經有缺損的情況下,使用硬性喉頭鏡則喉頭鏡會陷入該部位而位置關係會有所移動,因此會導致對喉頭撐開等造成障礙,或是傷及牙齦等等的疑慮。In any case, rigid laryngoscopes have the disadvantage of damaging teeth, lips, tongue, and oral cavity due to their rigid petioles, and even palate protrusion must be handled with caution. The less experienced the person is, the more likely they are to misunderstand psychologically when inserting the fixed curved petiole and bend the head back more forcefully, which can easily lead to damage to the cervical spine or teeth. Even in the case of a missing front tooth, the use of a rigid laryngoscope will cause the laryngoscope to sink into the area and the positional relationship will move, which may cause obstacles to the laryngeal opening, or damage to the gums.
從急救心肺復甦時的現場中施術的容易度來看,會有優先嘗試喉管或食道封閉式人工氣道的傾向,但隨著情況不同,有時候氣道確保會困難且需要重新插管之時間,相較於氣管插管,較無法完全保護氣道免於受到胃內容物之逆流/誤嚥因此會發生誤嚥,或是對食道氣管造成後遺症的事例偶而可見。氣管插管係為最確實的氣道確保手法,若可藉由簡便且迅速且可安全的氣管插管的產品之使用來降低氣管插管之施術的難易度,則可實現最速且最確實且效果高的急救心肺復甦之試行。From the perspective of the ease of performing the procedure on the spot during emergency CPR, there is a tendency to give priority to trying a laryngeal or esophageal closed artificial airway, but depending on the situation, sometimes it is difficult to secure the airway and time is required for reintubation. Compared with tracheal intubation, it is less likely to completely protect the airway from the reflux/misingestion of gastric contents, so misingestion may occur, or there may be cases where sequelae to the esophagus and trachea are occasionally seen. Tracheal intubation is the most reliable method to secure the airway. If the difficulty of tracheal intubation can be reduced by using products that are simple, quick, and safe for tracheal intubation, the fastest, most reliable, and most effective emergency CPR can be implemented.
在民眾做的急救心肺復甦時的現場中,AED(自動體外心臟電擊去顫器)的普及與受過使用法講習的經驗者逐漸變多,而被活用。反觀換氣(人工呼吸)則由於不存在自動機器因此都被忽視。關於都市部,由於想定急救隊抵達需要數分鐘左右因此以AED與胸骨壓迫(心臟按摩)為主的心肺復甦之試行被認為是妥當的,但在農山漁村地區或山間部離島等之非都市部中,可以想像急救隊的抵達與搬送需要相當的時間,而會有導致到院前時間拖長的疑慮。In the scene of emergency CPR performed by the public, AED (Automated External Cardiopulmonary Defibrillator) is becoming more and more popular and there are more and more people who have been trained in its use, so it is being used. On the other hand, ventilation (artificial respiration) is ignored because there is no automatic machine. In urban areas, it is considered appropriate to try CPR mainly based on AED and sternal compression (heart massage) because it is assumed that it will take several minutes for the emergency team to arrive. However, in non-urban areas such as rural and fishing villages or mountainous islands, it is conceivable that the arrival and transportation of the emergency team will take a considerable amount of time, and there is a concern that it will cause a delay in the time before the hospital.
尤其是在此情況下,除了AED與胸骨壓迫以外,相望能夠併用氣道確保、換氣。此狀況係在大規模的災害或戰亂時也是同樣地,簡便且迅速且可安全地進行氣管插管行為的產品之普及與以急救心肺復甦時為限而讓有資格民眾做活用,則人命救活之機會會增大,可期待血中氧濃度降低而失去的人命之救濟。Especially in this case, in addition to AED and sternal compression, airway securing and ventilation can be used simultaneously. This situation is also the same in large-scale disasters or wars. If products that can easily, quickly and safely perform tracheal intubation are popularized and qualified people are allowed to use them only during emergency cardiopulmonary resuscitation, the chances of saving lives will increase, and lives lost due to reduced blood oxygen concentration can be expected to be saved.
有鑑於以上的點,本發明的目的在於,藉由提供簡便且迅速並使安全的氣管插管成為可能的氣管插管裝置,以防止臨床醫療上的事故同時對氣管插管賦予迅速性和檢查性,進而帶來預後之改善。 [用以解決課題之手段]In view of the above points, the purpose of the present invention is to prevent clinical medical accidents by providing a tracheal intubation device that makes tracheal intubation simple, quick and safe, and to provide rapidity and inspection for tracheal intubation, thereby improving the prognosis.[Means for solving the problem]
本發明的氣管插管裝置,其特徵為, 具備: 氣管內管,係被插管至氣管內;和 插入部,係被插入至前記氣管內管中; 前記插入部係具有:在該插入部已被插入至前記氣管內管的狀態下,用來取得該氣管內管之尖端部附近之映像所需之觀察部,並且具備有作為將該氣管內管引導至氣管的通條之機能; 已被插入有前記插入部的前記氣管內管係: 在被插入至喉頭部為止以前,具有藉由前記插入部之整形而保持形狀的剛性; 在被插入至聲門深處並受到來自氣管之內壁的力的情況下,則具有變成沿著該內壁之形狀的柔軟性。The endotracheal intubation device of the present invention is characterized by: having: an endotracheal tube to be inserted into the trachea; and an insertion portion to be inserted into the endotracheal tube; the insertion portion has: an observation portion required for obtaining an image near the tip of the endotracheal tube when the insertion portion has been inserted into the endotracheal tube, and has a function as a rod for guiding the endotracheal tube to the trachea; the endotracheal tube into which the insertion portion has been inserted has: rigidity to maintain its shape by shaping the insertion portion until it is inserted into the laryngeal part; when inserted into the deep part of the glottis and subjected to a force from the inner wall of the trachea, has flexibility to change into a shape along the inner wall.
於本發明中,在進行氣管插管的情況下,在無負荷狀態下具有略為彎曲之狀態且可容易變形的氣管內管中,係被插入具有通條機能的插入部。此時,氣管內管,係藉由插入部之插入而被保持幾乎直線狀的形狀,且尖端部係可隨著施術者的多樣的意圖而被整形成任意之角度/形狀並維持該形狀。In the present invention, when tracheal intubation is performed, the insertion portion having a cleansing rod function is inserted into the endotracheal tube which has a slightly curved state and can be easily deformed in a no-load state. At this time, the endotracheal tube is kept in a nearly straight shape by the insertion of the insertion portion, and the tip portion can be shaped into an arbitrary angle/shape according to the operator's various intentions and maintain the shape.
在此狀態下,氣管內管的彈性/形狀恢復力與插入部的剛性係呈拮抗,因此只要未被施加足以破壞該拮抗狀態之外力,則該任意形狀就會被維持。然後,已被插入有插入部的氣管內管,係在維持著該整形形狀的狀態下,尖端部會抵達喉頭的聲門部,並且插入之。In this state, the elasticity/shape restoring force of the endotracheal tube and the rigidity of the insertion part are in antagonism, so the arbitrary shape will be maintained unless an external force sufficient to destroy the antagonism is applied. Then, the endotracheal tube with the insertion part inserted reaches the glottis of the larynx and is inserted while maintaining the shaped shape.
到此階段為止,插入部,係藉由其剛性而讓術者可將氣管內管引導致聲門部為止來做輔助的這點上,是和先前的通條發揮相同的機能。又,此時,藉由插入部尖端的觀察部所得的映像,係可輔助術者,讓其可將氣管內管的尖端,朝向經由氣管的聲門的方向而逐漸插入。Up to this stage, the insertion part, by its rigidity, assists the operator in guiding the endotracheal tube to the glottis, which is the same function as the previous cleaning rod. In addition, at this time, the image obtained by the observation part at the tip of the insertion part can assist the operator to gradually insert the tip of the endotracheal tube toward the glottis through the trachea.
其後,已被插入有插入部的氣管內管,係被插入至聲門深處然後一旦受到來自於氣管之直線狀之內壁的力,就會因為插入部的柔軟性,導致氣管內管的彈性力與插入部的內部應力之拮抗被破壞,變成沿著該內壁的形狀。然後繼續沿著內壁而被插入達到所定位置後,實施氣球的膨脹、或氣管內管之固定等之所定之措施,並且進行插入部從氣管內管的拔出,就完成氣管內管之插管。After that, the endotracheal tube with the inserted part is inserted to the deep part of the glottis and once it is subjected to the force from the linear inner wall of the trachea, the elastic force of the endotracheal tube and the internal stress of the inserted part are destroyed due to the softness of the inserted part, and the tube is changed into a shape along the inner wall. After the tube is inserted along the inner wall and reaches the predetermined position, the balloon is inflated or the endotracheal tube is fixed, and the inserted part is removed from the endotracheal tube, and the intubation of the endotracheal tube is completed.
此期間,根據藉由插入部尖端的觀察部所得的映像,就可謀求防止食道誤插管及單肺插管、或往氣管內管之正確位置的留置。又,插入部從氣管內管的拔出,係由於插入部是具有柔軟性,因此可毫無障礙地進行。During this period, the image obtained through the observation part at the tip of the insertion part can be used to prevent esophageal intubation and single lung intubation, or to place the endotracheal tube at the correct position. In addition, the insertion part can be removed from the endotracheal tube without any hindrance because the insertion part is flexible.
因此,若依據本發明,則藉由觀察部所得的映像就可監視著氣管內管的插管狀況,而不需要特別熟練,就能確實且容易地進行氣管內管之插管。藉此,可提供簡便且迅速並使安全的氣管插管成為可能的氣管插管裝置,可防止臨床醫療上的事故同時對氣管插管賦予迅速性和檢查性,進而帶來預後之改善。Therefore, according to the present invention, the intubation status of the endotracheal tube can be monitored by the image obtained by the observation part, and the endotracheal tube can be intubated reliably and easily without special skills. Thereby, a endotracheal intubation device that enables simple, rapid and safe endotracheal intubation can be provided, which can prevent clinical medical accidents and provide rapidity and inspection for endotracheal intubation, thereby improving the prognosis.
於本發明中,前記插入部係亦可具備:外被部,係具有可撓性的氟樹脂製或被施有氟樹脂被膜;和金屬護套部,係被插入至前記外被部,且可彎曲;和芯金部,係被插入至前記金屬護套部並用以容許該插入部之整形所致之彎曲;和傳送路,係被設在前記金屬護套部內並通往前記觀察部。In the present invention, the aforementioned insertion part may also include: an outer coating part, which is made of flexible fluororesin or coated with a fluororesin film; a metal sheath part, which is inserted into the aforementioned outer coating part and can be bent; a core metal part, which is inserted into the aforementioned metal sheath part and is used to allow bending caused by the shaping of the insertion part; and a transmission path, which is arranged in the aforementioned metal sheath part and leads to the aforementioned observation part.
據此,由於外被部是具有氟樹脂之表面,因此插入部對氣管內管的潤滑性較高,所以插入部對氣管內管之插入、或插入部從氣管內管的拔去,皆可滑順地進行。又,可將通往觀察部的傳送路,藉由金屬護套部而加以保護。又,主要是藉由芯金部,就可對插入部賦予身為通條之機能。According to this, since the outer sheath has a fluororesin surface, the insertion part has a high lubricity to the endotracheal tube, so the insertion part can be smoothly inserted into the endotracheal tube or removed from the endotracheal tube. In addition, the transmission path to the observation part can be protected by the metal sheath part. In addition, mainly by the core metal part, the insertion part can be given the function of a clean rod.
此情況下,前記金屬護套部,係亦可部分或全部是藉由,由形狀記憶合金或超彈性合金所形成的螺旋管,而被構成。In this case, the aforementioned metal sheath portion may also be partially or entirely formed by a spiral tube formed of a shape memory alloy or a superelastic alloy.
據此,螺旋管是由形狀記憶合金來形成的情況下,因為使用所產生的塑性變形而導致變得彎曲的螺旋管之部分,是可藉由再生消毒時等之加熱行為而發揮形狀記憶機能,而使其恢復成產品的初期形狀。Accordingly, when the spiral tube is formed of a shape memory alloy, the portion of the spiral tube that has become bent due to plastic deformation caused by use can be restored to the original shape of the product by exerting the shape memory function through heating during regeneration and sterilization.
又,藉由一般的金屬材料來形成螺旋管的情況下,則會因為施術時賦予給螺旋管的形狀變形,而導致螺旋管容易朝剖面方向壓扁而引發傳送路之斷裂等之憂慮,但藉由以超彈性合金來形成螺旋管,就可降低螺旋管的剖面方向之變形,防止斷裂。Furthermore, when the spiral tube is formed by ordinary metal materials, the shape deformation given to the spiral tube during the operation may cause the spiral tube to be easily flattened in the cross-sectional direction, causing concerns such as the rupture of the transmission path. However, by forming the spiral tube with a superelastic alloy, the deformation in the cross-sectional direction of the spiral tube can be reduced and the rupture can be prevented.
又,前記金屬護套部,係亦可部分或全部是藉由:對由鎳鈦合金、鈦或是鈦合金、或不鏽鋼所構成的管材,施以使其成為螺旋狀或是螺紋狀的加工、或賦予可撓性的加工而成的圓筒狀構件,而被構成。Furthermore, the aforementioned metal sheath portion may be partially or entirely formed by: processing a pipe made of nickel-titanium alloy, titanium or titanium alloy, or stainless steel to make it spiral or threaded, or to impart flexibility to the pipe to form a cylindrical member.
據此,可一面賦予可撓性,一面構成就結構而言可防止往橫剖面方向之挫曲或變形的金屬護套部。又,可容易地達成,已被插入有插入部的氣管內管所被要求的,上述之保持任意形狀的剛性與會變成沿著氣管內壁之形狀的柔軟性。According to this, a metal sheath portion can be provided with flexibility while being structurally prevented from buckling or deforming in the cross-sectional direction. Also, the rigidity required of an endotracheal tube into which the insertion portion has been inserted, and the flexibility required of the endotracheal tube to maintain an arbitrary shape and the flexibility required of the endotracheal tube to conform to a shape along the inner wall of the trachea can be easily achieved.
又,前記芯金部,係亦可由使用加工熱處理製程而被調質過的鈦或是鈦合金、或不鏽鋼所構成,且被包覆有氟系樹脂。據此,藉由適切地選擇這些金屬的硬度與形狀保持特性,就可更加容易地達成上記剛性及柔軟性。Furthermore, the front core metal part can also be made of titanium or titanium alloy or stainless steel that has been quenched and tempered using a heat treatment process and coated with a fluorine resin. Accordingly, by appropriately selecting the hardness and shape retention characteristics of these metals, it is easier to achieve the upper rigidity and flexibility.
又,前記外被部,係亦可由聚四氟乙烯(PTFE)或四氟乙烯/全氟烷氧基乙烯共聚樹脂(PFA)等之氟系樹脂所構成,或由以該氟系樹脂施予了表面皮膜的素材所構成。Furthermore, the outer covering mentioned above may be made of a fluorine-based resin such as polytetrafluoroethylene (PTFE) or tetrafluoroethylene/perfluoroalkoxyethylene copolymer (PFA), or a material having a surface film formed of the fluorine-based resin.
據此,可確實地提高上述的與氣管內管之潤滑性。亦即,上述的從氣管內管的插入部之拔出時,對於總體而言具有些許黏著性與摩擦性之矽膠系樹脂是被經常採用的氣管內管,可有效發揮最佳的潤滑性,可使拔去變得容易。使用其他素材的情況下,會產生阻力,想定會導致在氣管內管的留置場所之移動,或在拔出上需要多餘的時間等等。According to this, the lubricity with the endotracheal tube can be surely improved. That is, when the endotracheal tube is removed from the insertion portion, the silicone resin, which has a little stickiness and friction as a whole, is often used for the endotracheal tube, and can effectively exert the best lubricity, making it easy to remove. When other materials are used, resistance will be generated, which will surely cause the endotracheal tube to move at the indwelling site or require extra time for removal.
又,前記觀察部係亦可具備:照明手段,係用以照明前記氣管內管之尖端部之附近;和攝像元件,係用來取得該尖端部之附近之映像;或者亦可使用照明光傳送用及影像傳送用之光纖而被構成。據此,可容易地構成觀察部。Furthermore, the aforementioned observation section may also include: an illumination means for illuminating the vicinity of the tip of the aforementioned endotracheal tube; and an imaging element for acquiring an image of the vicinity of the tip; or may be constructed using optical fibers for transmitting illumination light and for transmitting images. Thus, the observation section can be easily constructed.
以下,使用圖式來說明本發明的實施形態。圖1係為本發明的一實施形態所述之氣管插管裝置的斜視圖。如圖1所示,該氣管插管裝置1係具備:被插管至插管對象者之氣管內的氣管內管2、和被插入至氣管內管2的插入部3。The following is a diagram to illustrate the embodiments of the present invention. Fig. 1 is a perspective view of an endotracheal intubation device according to an embodiment of the present invention. As shown in Fig. 1, the endotracheal intubation device 1 includes an endotracheal tube 2 inserted into the trachea of an intubation subject, and an insertion portion 3 inserted into the endotracheal tube 2.
氣管內管2係具有,在未被插入部3插入的無負荷狀態下,是以圓的1/3左右之部分而被構成的圓弧狀之形狀。氣管內管2,係在已被變形的情況下,會藉由其捲曲與素材之彈性,在無負荷時具有會恢復成圓弧狀之形狀的形狀恢復應力。The endotracheal tube 2 has an arc shape formed by about 1/3 of a circle in a no-load state when not inserted by the insertion portion 3. When the endotracheal tube 2 is deformed, it has a shape recovery stress that restores the shape to the arc shape when there is no load due to its curling and the elasticity of the material.
插入部3係具備在被插入至氣管內管2之狀態下用以取得氣管內管2之尖端部附近之映像所需之觀察部4,並且具備將氣管內管2引導至氣管所需之作為通條之機能。該通條之機能,係在插管手技時,氣管內管2之形狀除了尖端側之一部分以外,其餘都是呈直線狀為佳,因此係為被插入至氣管內管2而使氣管內管2整形成該形狀之機能。The insertion portion 3 has an observation portion 4 for obtaining an image of the vicinity of the tip of the endotracheal tube 2 when inserted into the endotracheal tube 2, and has a function as a cleaning rod for guiding the endotracheal tube 2 into the trachea. The function of the cleaning rod is that during the intubation technique, the shape of the endotracheal tube 2 is preferably a straight line except for a portion on the tip side, so the function of the cleaning rod is to be inserted into the endotracheal tube 2 and shape the endotracheal tube 2 into the shape.
已被插入有插入部3的氣管內管2,係在被插入至喉頭部為止以前,具有保持已被整形之形狀的剛性。亦即,此情況下,插入部3係發揮原本作為通條之機能。在圖1中係圖示,氣管內管2係被插入有插入部3,而呈現上記之任意形狀的狀態。The endotracheal tube 2 into which the insertion portion 3 has been inserted has the rigidity to maintain the reshaped shape until it is inserted into the laryngeal part. That is, in this case, the insertion portion 3 plays the original function of a cleaning rod. FIG. 1 shows a state in which the endotracheal tube 2 is inserted into the insertion portion 3 and presents the above-mentioned arbitrary shape.
另一方面,已被插入有插入部3的氣管內管2,係在被插入至聲門深處並受到來自氣管之直線狀之內壁的力的情況下,則具有變成沿著該內壁之形狀的柔軟性。亦即,此情況下,插入部3係不會使氣管內管2維持上記之任意形狀,而會使其變成沿著內壁之形狀而發揮機能。On the other hand, the endotracheal tube 2 into which the insertion portion 3 has been inserted has flexibility to change into a shape along the inner wall when it is inserted deep into the glottis and receives a force from the linear inner wall of the trachea. That is, in this case, the insertion portion 3 does not make the endotracheal tube 2 maintain the arbitrary shape mentioned above, but makes it function by changing into a shape along the inner wall.
圖2係圖示插入部3之剖面。如圖2所示,插入部3係具備:具有可撓性的氟樹脂製的或具有氟樹脂被膜的外被部5;和被插入至外被部5,並可彎曲的金屬護套部6;和被插入至金屬護套部6,容許插入部3之塑性變形所致之彎曲的芯金部7;和被設在金屬護套部6內,通往觀察部4的傳送路8。Fig. 2 is a cross-sectional view of the insertion part 3. As shown in Fig. 2, the insertion part 3 comprises: an outer sheath part 5 made of flexible fluororesin or having a fluororesin film; a metal sheath part 6 inserted into the outer sheath part 5 and capable of bending; a core metal part 7 inserted into the metal sheath part 6 and allowing bending due to plastic deformation of the insertion part 3; and a transmission path 8 provided in the metal sheath part 6 and leading to the observation part 4.
金屬護套部6,係部分或全部是藉由,由形狀記憶合金或超彈性合金所形成的螺旋管,而被構成。具體而言,金屬護套部6,係部分或全部是藉由:對由鎳鈦合金、鈦或是鈦合金、或不鏽鋼所構成的管材,施以使其成為螺旋狀或是螺紋狀的加工、或賦予可撓性的加工而成的圓筒狀構件,而被構成。The metal sheath part 6 is partially or entirely formed of a spiral tube formed of a shape memory alloy or a superelastic alloy. Specifically, the metal sheath part 6 is partially or entirely formed of a cylindrical member formed by processing a pipe made of nickel-titanium alloy, titanium or titanium alloy, or stainless steel to make it spiral or threaded, or to give it flexibility.
在本實施形態中,金屬護套部6,係在其尖端側與後端側,具有由所述之圓筒狀構件而被構成的尖端側螺旋管部9及後端側螺旋管部10。In this embodiment, the metal sheath portion 6 has a tip side spiral tube portion 9 and a rear end side spiral tube portion 10 formed of the above-mentioned cylindrical member on the tip side and the rear end side thereof.
外被部5,係由聚四氟乙烯(PTFE)或四氟乙烯/全氟烷氧基乙烯共聚樹脂(PFA)等之氟系樹脂所構成,或由以該氟系樹脂施予了表面皮膜的素材所構成。觀察部4係具備:照明手段,係用以照明氣管內管2之尖端部之附近;和攝像元件,係用來取得該尖端部之附近之映像。The outer cover 5 is made of a fluorine resin such as polytetrafluoroethylene (PTFE) or tetrafluoroethylene/perfluoroalkoxyethylene copolymer (PFA), or a material having a surface film formed of the fluorine resin. The observation section 4 includes: an illumination means for illuminating the vicinity of the tip of the endotracheal tube 2; and an imaging element for acquiring an image of the vicinity of the tip.
在插入部3之後端部係設有,用來防止插入部3從氣管內管2之尖端往插管對象者之體內露出的檔止器11。檔止器11,係為了使插入部3之後端部位於最佳位置,而被設有用來固定檔止器11所需之手動螺栓12。又,在插入部3之後端係設有,用來封閉該後端的封端蓋13。通往觀察部4的傳送路8,係經由封端蓋13而被導出至外部。A stopper 11 is provided at the rear end of the insertion portion 3 to prevent the insertion portion 3 from being exposed from the tip of the endotracheal tube 2 into the body of the intubated subject. The stopper 11 is provided with a manual bolt 12 required to fix the stopper 11 in order to position the rear end of the insertion portion 3 at the optimal position. In addition, a sealing cap 13 is provided at the rear end of the insertion portion 3 to seal the rear end. The transmission path 8 leading to the observation portion 4 is guided to the outside through the sealing cap 13.
於此構成中,將氣管內管2插管至插管對象者的氣管內之際,首先,在無負荷狀態下具有圓弧形狀且可容易彈性變形的氣管內管2中,將具有通條機能的插入部3進行插入,直到氣管內管2後端部之連接器14抵接於檔止器11為止。插入部3,係對氣管內管2,定位在不會從其尖端突出的最佳的插入位置,然後以手動螺栓12而被固定。In this configuration, when the endotracheal tube 2 is inserted into the trachea of the intubation subject, first, the insertion portion 3 having a cleaning rod function is inserted into the endotracheal tube 2 which has an arc shape and can be easily elastically deformed in a no-load state until the connector 14 at the rear end of the endotracheal tube 2 abuts against the stopper 11. The insertion portion 3 is positioned at the optimal insertion position for the endotracheal tube 2 so that it does not protrude from the tip thereof, and then fixed with the manual bolt 12.
此時,氣管內管2,係藉由插入部3之插入而被整形並保持成近乎直線狀。然後,已被插入有插入部3的氣管內管2,其尖端部會變成適合插入至處於嗅吸姿勢之插管對象者之喉頭部為止的任意形狀,插入部3會抵抗氣管內管2的形狀恢復力而將其整形。該任意形狀係為例如,尖端部是呈35°~90°左右彎曲的如圖1所示的形狀。At this time, the endotracheal tube 2 is shaped and maintained in a nearly straight shape by the insertion of the insertion portion 3. Then, the tip of the endotracheal tube 2 inserted with the insertion portion 3 becomes an arbitrary shape suitable for insertion into the larynx of the intubation subject in the sniffing posture, and the insertion portion 3 resists the shape restoring force of the endotracheal tube 2 and shapes it. The arbitrary shape is, for example, a shape in which the tip is bent at about 35° to 90° as shown in FIG. 1 .
在此狀態下,氣管內管2的形狀恢復力與插入部3的整形後之剛性係呈拮抗,因此只要未被施加足以破壞該拮抗狀態之外力,則氣管內管2的任意形狀就會被維持。然後,已被插入有插入部3的氣管內管2,係在被維持成該任意形狀的狀態下,尖端部會被插入至處於嗅吸姿勢的插管對象者15的喉頭之聲門部16為止。In this state, the shape restoring force of the endotracheal tube 2 and the rigidity of the reshaped insertion portion 3 are in antagonism, so unless an external force sufficient to destroy the antagonistic state is applied, the arbitrary shape of the endotracheal tube 2 is maintained. Then, the endotracheal tube 2 with the insertion portion 3 inserted therein is inserted until the tip portion is inserted into the
圖3係圖示已被插入有插入部3的氣管內管2,被插入至處於嗅吸姿勢的插管對象者15的喉頭之聲門部16為止時的狀態。在此狀態下,氣管內管2係被維持成上記任意形狀,氣管內管2的尖端部,係隨應於術者(手技者)之意圖而呈整形狀態。Fig. 3 shows a state where the endotracheal tube 2, into which the insertion portion 3 has been inserted, is inserted up to the
亦即,在此階段中,插入部3,係藉由其剛性而讓術者(手技者)將氣管內管2引導致聲門部16為止進行輔助,在這點上是發揮和先前的通條相同之機能。接著術者係將氣管內管2之尖端,往經由聲門17的方向繼續插入。此時,藉由插入部3尖端的觀察部4所得的映像,可謀求防止往食道18的誤插管及單肺插管。That is, at this stage, the insertion portion 3 assists the operator (surgeon) in guiding the endotracheal tube 2 to the
已被插入有插入部3的氣管內管2,係在其後,一旦被插入至聲門17深處而受到來自氣管19的直線狀之內壁20的力,就會因為柔軟性,導致維持整形形狀的拮抗關係被破壞,變成沿著內壁20之形狀。Once the endotracheal tube 2 having the inserted portion 3 is inserted deep into the
然後,已被插入有插入部3的氣管內管2,係沿著內壁20,而被插入至如圖4所示的所定位置為止,在進行氣球21的膨脹、或氣管內管2對插管對象者15的固定等之所定之處置後,進行插入部3從氣管內管2之拔出。Then, the endotracheal tube 2 having the inserted insertion portion 3 is inserted along the
該插入部3之拔出,係由於插入部3的外被部5,具有可撓性的氟樹脂製或是具有氟樹脂被膜,因此潤滑度佳,而可被容易地進行。藉由該插入部3之拔出,氣管內管2的尖端部就會留置在氣管19內。然後,插管對象者15係被擺成通常的仰臥位,插管就完成。圖4中係圖示了該插管完成時的狀態。The insertion part 3 can be easily removed because the outer cover 5 of the insertion part 3 is made of flexible fluororesin or has a fluororesin film, so it has good lubricity. By removing the insertion part 3, the tip of the endotracheal tube 2 is left in the
如以上所述,若依據本實施形態的氣管插管裝置1,則已被插入有插入部3的氣管內管2,係在插入至喉頭部(聲門部16)為止之際具有保持整形所致之任意形狀的剛性,在其後插入至聲門17深處之際係具有變成氣管19之沿著內壁20之形狀的柔軟性,因此可實現簡便且迅速且安全的氣管插管。As described above, according to the endotracheal intubation device 1 of this embodiment, the endotracheal tube 2 into which the insertion portion 3 has been inserted has the rigidity to maintain the arbitrary shape due to plastic surgery until it is inserted into the laryngeal part (glottis 16), and has the flexibility to change into the shape along the
亦即,已被插入有插入部3的氣管內管2,係可自由整形成任意之彎曲形狀而可容易實現順著術者所意圖之插管途徑的插管,並且一旦受到過大的力就會容易變形而可預防傷害之發生。That is, the endotracheal tube 2 having the insertion portion 3 inserted therein can be freely shaped into any curved shape and can easily be intubated along the intubation path intended by the operator, and can easily be deformed once subjected to excessive force to prevent the occurrence of injuries.
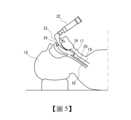
又,如圖5所示,先前的硬性喉頭鏡22,係硬質葉柄23是接觸於上顎前齒24,以上顎前齒24作為支點才能作用,存有此一結構上、物理上的缺點,而且硬質葉柄23容易與牙齒或口腔內組織接觸,相對於此,若依據氣管插管裝置1,藉由上記順著所意圖之插管途徑的插管與變形容易性(柔軟性),對於牙齒缺損或有搖動齒等的插管對象者15,也可容易地遂行插管手技。Furthermore, as shown in FIG. 5 , the previous
又,在復甦時等需要緊急插管但牙齒狀態不佳的情況下也是,由於適用條件為較廣範圍,因此可毫無猶豫地執行插管手技。尤其是,在邁向高齡化的各國中,牙齒缺損或牙齒狀態不佳的要救護者會增加,因此被認為是有用的。In addition, even in cases where emergency intubation is required during resuscitation and the teeth are in poor condition, the applicable conditions are wide, so intubation can be performed without hesitation. In particular, in countries with an aging population, the number of people who need rescue due to tooth loss or poor teeth is increasing, so this is considered useful.
又,插入部3,係具備上述的外被部5、金屬護套部6、芯金部7、及傳送路8,因此對氣管內管2的插入部3之插入、或插入部3已被插入至氣管內管2之狀態下的插入部3及氣管內管2之塑性變形、從氣管內管2的插入部3之拔出,都可滑順地進行。Furthermore, the insertion portion 3 comprises the outer covering portion 5, the metal sheath portion 6, the core metal portion 7, and the transmission path 8, so that the insertion portion 3 of the endotracheal tube 2, the plastic deformation of the insertion portion 3 and the endotracheal tube 2 when the insertion portion 3 has been inserted into the endotracheal tube 2, and the removal of the insertion portion 3 from the endotracheal tube 2 can be smoothly performed.
又,可將通往觀察部4的傳送路8,藉由金屬護套部6而加以保護。又,主要是藉由芯金部7,就可對插入部3賦予身為通條之機能。Furthermore, the transmission path 8 leading to the observation part 4 can be protected by the metal sheath part 6. Furthermore, mainly by the core metal part 7, the insertion part 3 can be given the function of a cleaning rod.
又,金屬護套部6的部分或全部,是藉由形狀記憶合金所形成的螺旋管而被構成的情況下,則因使用而發生塑性變形而彎曲的螺旋管之部分,是可藉由插入部3的消毒時等之加熱而使形狀記憶合金發揮形狀記憶機能,而恢復成初期之形狀。Furthermore, when part or all of the metal sheath portion 6 is constructed by a spiral tube formed of a shape memory alloy, the portion of the spiral tube that is plastically deformed and bent due to use can be restored to its initial shape by heating the insertion portion 3 during disinfection, etc., so that the shape memory alloy can exert its shape memory function.
又,金屬護套部6的部分或全部之螺旋管,是以一般的金屬材料而被形成的情況下,則會因為施術時賦予給螺旋管的形狀變形,而導致螺旋管容易朝剖面方向壓扁而引發傳送路8之斷裂等之憂慮,但螺旋管是以超彈性合金而被形成的情況下,就可降低螺旋管的剖面方向之變形,可防止傳送路8之斷裂。Furthermore, if part or all of the spiral tube of the metal sheath portion 6 is formed of a general metal material, the shape deformation imparted to the spiral tube during the operation may cause the spiral tube to be easily flattened in the cross-sectional direction, thereby causing concerns such as rupture of the transmission path 8. However, if the spiral tube is formed of a superelastic alloy, the deformation of the spiral tube in the cross-sectional direction can be reduced, thereby preventing the transmission path 8 from rupture.
又,關於金屬護套部6的部分或全部,係為對以鎳鈦合金等所構成之管材,施以使其變成螺旋狀等之加工而成的圓筒形狀之構件所構成,因此具有可撓性,同時結構上可防止往橫剖面方向之挫曲或變形。又,可容易地達成,已被插入有插入部3的氣管內管2所被要求的,上述之保持任意形狀的剛性、與會變成沿著氣管19之內壁20之形狀的柔軟性。In addition, part or all of the metal sheath 6 is formed of a cylindrical member formed by processing a pipe made of nickel-titanium alloy or the like into a spiral shape, so that it has flexibility and can prevent buckling or deformation in the cross-sectional direction. In addition, the rigidity required of the endotracheal tube 2 into which the insertion portion 3 is inserted, and the flexibility to conform to the shape of the
又,芯金部7,係由使用加工熱處理製程而被調質過的鈦或是鈦合金、或不鏽鋼所構成,且被包覆有氟系樹脂,因此藉由適切地選定、調整這些金屬的硬度與形狀保持特性,就可在極廣範圍的選項中選擇出上述的剛性及柔軟性,可隨應於術者的嗜好或所使用的氣管內管2之特性來做提供,因此尤其適合於實用。Furthermore, the core metal portion 7 is made of titanium or titanium alloy or stainless steel that has been tempered using a heat treatment process and is coated with a fluorine-based resin. Therefore, by appropriately selecting and adjusting the hardness and shape retention properties of these metals, the above-mentioned rigidity and flexibility can be selected from a wide range of options, and can be provided according to the operator's preference or the characteristics of the endotracheal tube 2 used, so it is particularly suitable for practical use.
又,外被部5,係由氟系樹脂或是以該氟系樹脂施以表面皮膜的素材所構成,因此可確實提高與氣管內管2之潤滑性。藉此,插入部3從氣管內管2的拔出之際,對於總體而言具有些許黏著性與摩擦性之矽膠系樹脂是被經常採用的氣管內管2,可有效發揮最佳的潤滑性,可使拔去變得容易。Furthermore, the outer covering 5 is made of fluorine-based resin or a material with a surface film of the fluorine-based resin, so that the lubricity with the endotracheal tube 2 can be surely improved. Thus, when the insertion part 3 is pulled out from the endotracheal tube 2, the silicone-based resin, which generally has a little stickiness and friction, is commonly used for the endotracheal tube 2, and the best lubricity can be effectively exerted, making the removal easier.
又,觀察部4係具備:照明手段,係用以照明氣管內管2之尖端部之附近;和攝像元件,係用來取得該尖端部之附近之映像;因此可提供明瞭的觀察。Furthermore, the observation section 4 is provided with: an illumination means for illuminating the vicinity of the tip end of the endotracheal tube 2; and an imaging element for acquiring an image of the vicinity of the tip end; thus, clear observation can be provided.
此外,本發明係不限定於上述的實施形態。例如,觀察部4係亦可使用照明光傳送用及影像傳送用之光纖來構成。此情況下,與觀察部4是由照明手段或攝像元件來構成的情況不同,具有不會發熱之優點。又,氣管插管裝置1,係即使在進行經鼻氣管插管的情況下,也可享有和經口氣管插管之情況相同之優點而做利用。In addition, the present invention is not limited to the above-mentioned embodiments. For example, the observation section 4 may be formed by using optical fibers for transmitting illumination light and images. In this case, unlike the case where the observation section 4 is formed by illumination means or an imaging element, there is an advantage that heat is not generated. Furthermore, the tracheal intubation device 1 can be used to enjoy the same advantages as the case of oral tracheal intubation even when performing nasotracheal intubation.
1:氣管插管裝置 2:氣管內管 3:插入部 4:觀察部 5:外被部 6:金屬護套部 7:芯金部 8:傳送路 9:尖端側螺旋管部 10:後端側螺旋管部 11:檔止器 12:手動螺栓 13:封端蓋 14:連接器 15:插管對象者 16:聲門部 17:聲門 18:食道 19:氣管 20:內壁 21:氣球 22:硬性喉頭鏡 23:硬質葉柄 24:上顎前齒1: Tracheal intubation device2: Endotracheal tube3: Insertion part4: Observation part5: Outer sheath6: Metal sheath7: Core metal part8: Transmission path9: Tip spiral tube part10: Back spiral tube part11: Stopper12: Manual bolt13: End cap14: Connector15: Intubation subject16: Glottis17: Glottis18: Esophagus19: Trachea20: Inner wall21: Balloon22: Rigid laryngoscope23: Rigid petiole24: Front teeth of maxillary jaw
[圖1]本發明的一實施形態所述之氣管插管裝置的模式性圖示的斜視圖。 [圖2]圖1的氣管插管裝置的橫剖面圖。 [圖3]用來說明圖1的氣管插管裝置中的已被插入有插入部的氣管內管,被插入至處於嗅吸姿勢的插管對象者的喉頭的聲門部時的狀態的說明圖。 [圖4]圖1的氣管插管裝置所致之插管手技完成時之狀態的模式圖。 [圖5]在硬性喉頭鏡中,使硬質葉柄接觸於上顎前齒,以其為支點才能作用而具有結構上、物理上之缺點的圖示。[Figure 1] A schematic oblique view of an endotracheal intubation device according to an embodiment of the present invention.[Figure 2] A cross-sectional view of the endotracheal intubation device of Figure 1.[Figure 3] An explanatory diagram for explaining the state of the endotracheal tube with the insertion portion inserted in the endotracheal intubation device of Figure 1 when it is inserted into the glottis of the larynx of the intubation subject in the sniffing position.[Figure 4] A schematic diagram of the state when the intubation technique is completed by the endotracheal intubation device of Figure 1.[Figure 5] An illustration of the structural and physical defects of a rigid laryngoscope in which the rigid petiole is brought into contact with the front teeth of the maxilla and can only function with it as a fulcrum.
1:氣管插管裝置1: Tracheal intubation device
2:氣管內管2: Endotracheal tube
3:插入部3: Insertion part
4:觀察部4: Observation Department
5:外被部5: Outer cover
6:金屬護套部6:Metal sheath part
8:傳送路8: Transmission path
9:尖端側螺旋管部9: Spiral tube part on the tip side
10:後端側螺旋管部10: Spiral tube at the rear end
11:檔止器11: Stopper
12:手動螺栓12: Manual bolts
13:封端蓋13: End cap
14:連接器14: Connector
Claims (7)
Translated fromChineseApplications Claiming Priority (2)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| JP2022175812AJP7379761B1 (en) | 2022-11-01 | 2022-11-01 | Tracheal intubation device |
| JP2022-175812 | 2022-11-01 |
Publications (2)
| Publication Number | Publication Date |
|---|---|
| TW202419115A TW202419115A (en) | 2024-05-16 |
| TWI850139Btrue TWI850139B (en) | 2024-07-21 |
Family
ID=88729086
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| TW112141709ATWI850139B (en) | 2022-11-01 | 2023-10-31 | Endotracheal tube device |
Country Status (3)
| Country | Link |
|---|---|
| JP (1) | JP7379761B1 (en) |
| TW (1) | TWI850139B (en) |
| WO (1) | WO2024095671A1 (en) |
Families Citing this family (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| CN120053858A (en)* | 2025-04-28 | 2025-05-30 | 广州灵云医疗科技有限公司 | Auxiliary intubation device |
Citations (6)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| JPH09238897A (en)* | 1996-03-13 | 1997-09-16 | Nippon Koden Corp | Endotracheal tube intubation endoscope |
| JP2000139818A (en)* | 1998-11-10 | 2000-05-23 | Nippon Koden Corp | Endoscope for endotracheal tube intubation |
| US20120304984A1 (en)* | 2011-05-31 | 2012-12-06 | Nellcor Puritan Bennett Llc | Reverse tracheal stoma dilation method and apparatus |
| CN104043172A (en)* | 2013-03-15 | 2014-09-17 | 成都嘉逸科技有限公司 | Endotracheal tube with memory alloy stent |
| CN206463314U (en)* | 2016-10-20 | 2017-09-05 | 赖欣 | Intracavitary closure type single-chamber bronchial cannula |
| CN112353358A (en)* | 2020-11-26 | 2021-02-12 | 郴州市第一人民医院 | Visual bronchoscope |
Family Cites Families (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| JPH11113843A (en)* | 1997-10-08 | 1999-04-27 | Nippon Koden Corp | Stylet with observation optics for endotracheal tube intubation |
| JP3309215B2 (en)* | 1998-10-20 | 2002-07-29 | 日本光電工業株式会社 | Endoscope for endotracheal tube intubation |
- 2022
- 2022-11-01JPJP2022175812Apatent/JP7379761B1/enactiveActive
- 2023
- 2023-10-04WOPCT/JP2023/036263patent/WO2024095671A1/ennot_activeCeased
- 2023-10-31TWTW112141709Apatent/TWI850139B/enactive
Patent Citations (6)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| JPH09238897A (en)* | 1996-03-13 | 1997-09-16 | Nippon Koden Corp | Endotracheal tube intubation endoscope |
| JP2000139818A (en)* | 1998-11-10 | 2000-05-23 | Nippon Koden Corp | Endoscope for endotracheal tube intubation |
| US20120304984A1 (en)* | 2011-05-31 | 2012-12-06 | Nellcor Puritan Bennett Llc | Reverse tracheal stoma dilation method and apparatus |
| CN104043172A (en)* | 2013-03-15 | 2014-09-17 | 成都嘉逸科技有限公司 | Endotracheal tube with memory alloy stent |
| CN206463314U (en)* | 2016-10-20 | 2017-09-05 | 赖欣 | Intracavitary closure type single-chamber bronchial cannula |
| CN112353358A (en)* | 2020-11-26 | 2021-02-12 | 郴州市第一人民医院 | Visual bronchoscope |
Also Published As
| Publication number | Publication date |
|---|---|
| TW202419115A (en) | 2024-05-16 |
| JP2024066309A (en) | 2024-05-15 |
| JP7379761B1 (en) | 2023-11-15 |
| WO2024095671A1 (en) | 2024-05-10 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| US6662804B2 (en) | Tracheostomy tube with cuff on inner cannula | |
| EP4183437A1 (en) | Visual laryngoscope/visual guide core-combined dual-visualization and dual-positioning tracheal intubation set | |
| Baker et al. | Equipment to manage a difficult airway during anaesthesia | |
| TWI850139B (en) | Endotracheal tube device | |
| WO2019162024A1 (en) | Snorkel ventilating airway and bite-block | |
| Dörges | Airway management in emergency situations | |
| CN111803773A (en) | Video laryngoscope and visual guide core combination dual visual dual positioning endotracheal intubation set | |
| Wittels | Basic airway management in adults | |
| Higginson | Respiratory assessment in critically ill patients: airway and breathing | |
| Davies et al. | Airway management | |
| Higginson et al. | Airway management for nurses: emergency assessment and care | |
| RU125472U1 (en) | CONNECTOR USED FOR BRONCHOSCOPY | |
| Wijdicks | Short of breath, short of air, short of mechanics | |
| Sagar et al. | Comparison of Supraglottic Devices I-gel and LMA Fastrach R as Conduit for Endotracheal Intubation | |
| Jindal et al. | Safety and efficacy of insertion of supraglottic devices in anaesthetised patients by first-time users | |
| JP3043337U (en) | Endoscopic stylet for endotracheal intubation | |
| Higginson et al. | Emergency and intensive care: assessing and managing the airway | |
| Armstrong et al. | Airway management in trauma | |
| Goodrich | 2 Endotracheal Intubation AP | |
| Pickford-Brake et al. | How to ensure safe airway suctioning and management for adults and children | |
| HAGBERG | SONIA VAIDA, HELEN A. LINDSAY, TIM M. COOK, LUIS GAITINI, AND | |
| Myatra et al. | Supraglottic Airway Devices | |
| Pearce | Single use, disposable | |
| Verma et al. | Malpositioned LMA confused as foreign body in nasal cavity | |
| Hopkin | Endotracheal Intubation |