RU2460494C2 - Endoprosthesis for sutureless intraabdominal plasty in case of ventral hernias - Google Patents
Endoprosthesis for sutureless intraabdominal plasty in case of ventral herniasDownload PDFInfo
- Publication number
- RU2460494C2 RU2460494C2RU2010124471/14ARU2010124471ARU2460494C2RU 2460494 C2RU2460494 C2RU 2460494C2RU 2010124471/14 ARU2010124471/14 ARU 2010124471/14ARU 2010124471 ARU2010124471 ARU 2010124471ARU 2460494 C2RU2460494 C2RU 2460494C2
- Authority
- RU
- Russia
- Prior art keywords
- endoprosthesis
- film
- central part
- mesh
- holes
- Prior art date
Links
Images



Landscapes
- Prostheses (AREA)
Abstract
Description
Translated fromRussianИзобретение относится к области медицины, а именно к хирургии, предназначено для выполнения атензионной интраабдоминальной пластики при вентральных грыжах и может найти широкое применение в оперативном лечении пациентов с грыжами.The invention relates to medicine, namely to surgery, is intended to perform atenzia intraabdominal plastic surgery for ventral hernias and can be widely used in surgical treatment of patients with hernias.
Проблема хирургического лечения грыж весьма актуальна в настоящее время, что связано с ростом грыженосительства среди населения. Несмотря на накопленный опыт в этой области, по причине высокого процента неудовлетворенностью результатами оперативного лечения послеоперационных вентральных грыж, больших паховых грыж, особенно рецидивных, поиски оптимальных решений продолжаются. В последние десятилетия техника оперативного лечения была пересмотрена. Одним из самых современных способов реконструкции брюшной стенки является интраабдоминальная (интраперитонеальная) пластика [1, 4, 5, 8] с применением многослойного эндопротеза, который помещают в брюшную полость и фиксируют непосредственно к брюшной стенке со стороны брюшины. Способ отличает простота, надежность (наименьшая частота рецидивов), повторяемость. При интраабдоминальной имплантации эндопротез контактирует с органами брюшной полости, поэтому для данного способа реконструкции брюшной стенки используют многослойный эндопротез. Указанный эндопротез имеет несколько слоев с различными свойствами поверхностей, которые скреплены между собой. Один из слоев прилегает к брюшной стенке, а другой слой безопасно контактирует с органами брюшной полости.The problem of surgical treatment of hernias is very relevant at the present time, which is associated with an increase in hernia carriage among the population. Despite the experience gained in this area, due to the high percentage of dissatisfaction with the results of surgical treatment of postoperative ventral hernias, large inguinal hernias, especially recurrent, the search for optimal solutions continues. In recent decades, the technique of surgical treatment has been revised. One of the most modern methods for reconstruction of the abdominal wall is intra-abdominal (intraperitoneal) plastic [1, 4, 5, 8] using a multilayer endoprosthesis, which is placed in the abdominal cavity and fixed directly to the abdominal wall from the side of the peritoneum. The method is distinguished by simplicity, reliability (the lowest frequency of relapse), repeatability. During intra-abdominal implantation, the endoprosthesis contacts the abdominal organs, therefore, for this method of reconstruction of the abdominal wall, a multilayer endoprosthesis is used. The specified endoprosthesis has several layers with various surface properties that are bonded to each other. One of the layers is adjacent to the abdominal wall, and the other layer is in safe contact with the abdominal organs.
Известны многослойные эндопротезы для пластики брюшной стенки (US 6171318, HERNIA MESH PATCH WITH STIFFENNING LAYER, US 6383201, SURGICAL PROTHESIS FOR REPAIRING A HERNIA), однако указанные эндопротезы имеют существенные недостатки. В ходе операции эндопротез фиксируется исключительно стандартными методами фиксации в тканях брюшной стенки - путем наложения швов по периферии. Установлено, что при данном способе оперативного лечения стандартная фиксация швами имеет ряд недостатков. Лигатуры создают зоны натяжения, силу которых трудно дозировать, особенно при повышении внутрибрюшного давления. Нить приобретает "пилящие" свойства, создает избыточное повреждение в зонах фиксации [2, 3]. Это может иногда привести к прорезыванию лигатур, смещению эндопротеза и рецидиву грыжи [10]. Прорезывание одного или нескольких швов ведет к отслаиванию эндопротеза от тканей брюшной стенки, что требует повторного вмешательства. Также в экспериментальных работах показано, что в зоне наложения швов наиболее выражен воспалительный процесс, что является причиной образования грубых рубцов и спаек [7]. Применяемые в хирургии многослойные эндопротезы изготовлены из полипропилена, который по своим физико-химическим свойствам является термопластом. Данный материал не обладает памятью формы и часто деформируется и смещается в пространстве в процессе эксплуатации, сокращается в размерах на 30% в течение года, что приводит к рецидиву. Тканевая реакция на эндопротез протекает по типу асептического воспаления и в ряде случаев заканчивается серомой, а затем нагноением.Multilayer endoprostheses for abdominal wall plasty are known (US 6171318, HERNIA MESH PATCH WITH STIFFENNING LAYER, US 6383201, SURGICAL PROTHESIS FOR REPAIRING A HERNIA), however, these endoprostheses have significant disadvantages. During the operation, the endoprosthesis is fixed exclusively by standard methods of fixation in the tissues of the abdominal wall - by suturing along the periphery. It was found that with this method of surgical treatment, standard fixation with sutures has several disadvantages. Ligatures create tension zones, the strength of which is difficult to dose, especially with an increase in intra-abdominal pressure. The thread acquires "sawing" properties, creates excessive damage in the fixation zones [2, 3]. This can sometimes lead to eruption of ligatures, displacement of the endoprosthesis and hernia recurrence [10]. The eruption of one or more sutures leads to flaking of the endoprosthesis from the tissues of the abdominal wall, which requires repeated intervention. It has also been shown in experimental works that the inflammatory process is most pronounced in the suturing area, which causes the formation of rough scars and adhesions [7]. Multilayer endoprostheses used in surgery are made of polypropylene, which by its physicochemical properties is a thermoplastic. This material does not have a shape memory and is often deformed and displaced in space during operation, is reduced in size by 30% during the year, which leads to relapse. The tissue reaction to the endoprosthesis proceeds as an aseptic inflammation and in some cases ends with seroma, and then suppuration.
Помимо многослойных эндопротезов для пластики брюшной стенки известен эндопротез (РФ №73780, СЕТЧАТЫЙ ЭНДОПРОТЕЗ ДЛЯ ПЛАСТИКИ ПЕРЕДНЕЙ БРЮШНОЙ СТЕНКИ), предназначенный для решения иной задачи: бесшовной пластики передней брюшной стенки. Изобретение, описанное в патенте РФ №73780, является наиболее близким по технической сущности к заявленному изобретению, поэтому его авторы принимают за прототип.In addition to multilayer endoprostheses for abdominal wall plasty, an endoprosthesis is also known (RF No. 73780, GRID ENDOPROTHESIS FOR PLASTIC FRONT ABDOMINAL WALL), designed to solve a different problem: seamless plastic surgery of the anterior abdominal wall. The invention described in the patent of the Russian Federation No. 73780, is the closest in technical essence to the claimed invention, therefore, its authors take as a prototype.
Конструкция прототипа состоит из центральной части в виде монолитной сетчатой пластины и периферийной части в виде монолитных полосок (лучей), расположенных радиально от геометрического центра конструкции, причем края полосок имеют пилообразную форму. Монолитные полоски (лучи) служат для фиксации устройства в брюшной стенке в ходе операции. Прототип изготавливается из пространственно-сшитого полимера, полученного путем фотополимеризации олигомеров метакрилового ряда. Отличительной особенностью такого способа производства является то, что процесс формирования изделия исключает какое-либо механическое воздействие на эндопротез. Любое механическое воздействие на полимер, как известно, провоцирует образование свободных радикалов, которые впоследствии приводят к деструкции полимера и нежелательным токсическим реакциям. Указанный полимерный материал является биологически инертным, не вызывает воспалительных реакций или реакции отторжения. Но, к сожалению, материал прототипа не обладает высокими показателями разрывной нагрузки, что ограничивает его применение для пластики брюшной стенки по поводу больших вентральных грыж. Также прототип имеет недостаток конструктивного решения. Дело в том, что наибольшая разрывная нагрузка приходится на места соединения лучей с центральной частью эндопротеза, которые имеют одинаковую ширину на всем своем протяжении. Именно в этом месте может произойти отрыв фиксирующих элементов-лучей от центральной части. При интраабдоминальной имплантации это чревато опасными осложнениями, например ущемлением петли кишки между сеткой и брюшной стенкой при отрыве луча. Кроме того, указанный эндопротез имеет одинаковые поверхности, в то время как свойства поверхностей эндопротеза для интраабдоминальной имплантации должны принципиально отличаться [6, 9].The design of the prototype consists of a central part in the form of a monolithic mesh plate and a peripheral part in the form of monolithic strips (rays) located radially from the geometric center of the structure, the edges of the strips having a sawtooth shape. Monolithic strips (rays) serve to fix the device in the abdominal wall during surgery. The prototype is made of a spatially cross-linked polymer obtained by photopolymerization of methacrylic oligomers. A distinctive feature of this method of production is that the process of product formation eliminates any mechanical effect on the endoprosthesis. Any mechanical effect on the polymer is known to provoke the formation of free radicals, which subsequently lead to polymer degradation and undesirable toxic reactions. The specified polymer material is biologically inert, does not cause inflammatory reactions or rejection reactions. But, unfortunately, the material of the prototype does not have high breaking load, which limits its use for plastic surgery of the abdominal wall due to large ventral hernias. Also, the prototype has the disadvantage of a constructive solution. The fact is that the greatest breaking load falls on the junction of the rays with the central part of the endoprosthesis, which have the same width along its entire length. It is in this place that the detachment of the fixing elements-rays from the central part can occur. With intra-abdominal implantation, this is fraught with dangerous complications, for example, infringement of the intestinal loop between the mesh and the abdominal wall when the beam is separated. In addition, the specified endoprosthesis has the same surfaces, while the properties of the surfaces of the endoprosthesis for intra-abdominal implantation should be fundamentally different [6, 9].
Техническая задача - создание прочного, надежно фиксируемого, многослойного эндопротеза для бесшовной атензионной интраабдоминальной пластики по поводу вентральных грыж из материала, который является биостабильным биосовместимым реактопластом.The technical problem is the creation of a durable, securely fixed, multilayer endoprosthesis for a seamless atensional intra-abdominal plastic surgery for ventral hernias from a material that is a biostable biocompatible thermoset.
Технический результат достигается тем, что эндопротез для бесшовной интраабдоминальной пластики при вентральных грыжах, центральная и периферийная части которого выполнены из пространственно-сшитого полимера путем фотополимеризации олигомеров метакрилового ряда, при этом периферийная часть выполнена в виде монолитных полосок, соединенных с центральной частью, укреплен полипропиленовой нитью, монолитные полоски периферийной части имеют отверстия и наибольшую ширину в местах соединения с центральной частью и расположены диаметрально, центральная часть образует монолитную систему, состоящую из пленки и сетки, соединенных между собой по диаметрально расположенным относительно геометрического центра центральной части двойным полоскам, средняя часть которых образует канал между пленкой и сеткой, одна поверхность гладкая и предназначена для контакта с органами брюшной полости, а другая - шероховатая или содержит рельефный рисунок, на протяжении полоски полипропиленовая нить прошнурована через отверстия, у основания нить входит в канал, протянута до основания противоположной полоски, где выходит и прошнурована через отверстия противоположной полоски. Центральная часть состоит из сетки и пленки одинаковой прямоугольной с закругленными краями формой с длинной сторон от 50 до 400 мм и окантовкой по периметру шириной от 1 до 3 мм. Сетка с шестигранными, или прямоугольными, или треугольными, или круглыми ячейками размером от 1 до 5 мм и шириной полимерной части между ячейками от 0,2 до 2 мм имеет толщину от 0,2 до 1 мм и предназначена для контакта с брюшной стенкой. Пленка толщиной от 0,2 до 1 мм имеет одну сторону шероховатую или содержащую рельефный рисунок, образующий элемент которого представляет собой шестиугольник, или прямоугольник, или треугольник, мультиплицированный по всей поверхности таким образом, что каждая сторона образующего элемента является общей стороной с соседствующим элементом, причем диаметр окружности, описанной вокруг образующего элемента рельефного рисунка, больше диаметра окружности, описанной вокруг ячейки сетки. Другая сторона пленки - гладкая и предназначена для контакта с органами брюшной полости. Центральная часть образует монолитную систему, состоящую из пленки и сетки, соединенных между собой по диаметрально расположенным относительно геометрического центра центральной части двойным полоскам. Толщина двойных полосок, соединяющих пленку с сеткой, от 0,2 до 1 мм. Средняя часть двойных полосок образует канал между пленкой и сеткой, по которому проходит полипропиленовая нить, которая в периферийной части прошнурована через отверстия, содержащиеся на диаметрально противоположных монолитных полосках периферийной части. Монолитные полоски периферийной части имеют пилообразную форму, что гарантирует их надежное удержание в тканях, предотвращает смещение эндопротеза относительно дефекта в брюшной стенке и позволяет отказаться от наложения швов. Для изготовления имплантата синтезирован полимерный материал, полученный в результате фотополимеризации олигомеров метакрилового ряда по патенту РФ №2309781 (приоритет от 25.05.2006). Применение в качестве материала пространственно-сшитого полимера исключает деформацию эндопротеза, обеспечивает надежность операции и благоприятное течение репаративного процесса.The technical result is achieved by the fact that the endoprosthesis for seamless intra-abdominal plastic surgery for ventral hernias, the central and peripheral parts of which are made of a spatially cross-linked polymer by photopolymerization of methacrylic series oligomers, while the peripheral part is made in the form of monolithic strips connected to the central part, is reinforced with a polypropylene thread monolithic strips of the peripheral part have holes and the greatest width at the junctions with the central part and the diametrically located but, the central part forms a monolithic system consisting of a film and a grid connected by double strips diametrically located relative to the geometric center of the central part, the middle part of which forms a channel between the film and the grid, one surface is smooth and is intended for contact with abdominal organs, and the other is rough or embossed, the polypropylene thread is laced through the holes along the strip, at the base the thread enters the channel, stretched to the base the opposite strip, where it comes out and is laced through the holes of the opposite strip. The central part consists of a grid and a film of the same rectangular shape with rounded edges with a shape from 50 to 400 mm long and edges around the perimeter with a width of 1 to 3 mm. A mesh with hexagonal, or rectangular, or triangular, or round cells from 1 to 5 mm in size and a polymer part between cells from 0.2 to 2 mm wide has a thickness of 0.2 to 1 mm and is intended for contact with the abdominal wall. A film with a thickness of 0.2 to 1 mm has one side, rough or containing a relief pattern, the forming element of which is a hexagon, or a rectangle, or a triangle, multiplied over the entire surface so that each side of the forming element is a common side with the neighboring element, moreover, the diameter of the circle described around the forming element of the relief pattern is larger than the diameter of the circle described around the mesh cell. The other side of the film is smooth and is intended for contact with the organs of the abdominal cavity. The central part forms a monolithic system consisting of a film and a grid connected by double strips diametrically located relative to the geometric center of the central part. The thickness of the double strips connecting the film to the grid is from 0.2 to 1 mm. The middle part of the double strips forms a channel between the film and the network through which the polypropylene thread passes, which is laced in the peripheral part through holes contained in diametrically opposite monolithic strips of the peripheral part. The monolithic strips of the peripheral part have a sawtooth shape, which guarantees their reliable retention in the tissues, prevents the endoprosthesis from shifting relative to the defect in the abdominal wall and eliminates suturing. For the manufacture of an implant, a polymer material was synthesized, obtained by photopolymerization of methacrylic oligomers according to the patent of the Russian Federation No. 2309781 (priority from 05.25.2006). The use of a spatially cross-linked polymer as a material eliminates the deformation of the endoprosthesis, ensures reliable operation and a favorable course of the reparative process.
Изобретение поясняется графическим материалом.The invention is illustrated by graphic material.
Фигура 1 - общий вид эндопротеза.Figure 1 - General view of the endoprosthesis.
Центральная часть (1) состоит из сетки и пленки прямоугольной формы с закругленными краями, где:The central part (1) consists of a grid and a film of rectangular shape with rounded edges, where:
А - от 50 до 400 мм;A - from 50 to 400 mm;
В - от 50 до 400 мм;B - from 50 to 400 mm;
2 - окантовка по периметру сетки и пленки шириной от 1 до 3 мм;2 - edging around the perimeter of the mesh and film with a width of 1 to 3 mm;
Сетку и пленку соединяют двойные сплошные полоски (3), образуя между сеткой и пленкой канал, содержащий полипропиленовую нить (5). Периферийная часть (4) в виде монолитных полосок - лучей длиной С - от 50 до 150 мм служат для фиксации устройства в брюшной стенке в ходе операции. Края лучей имеют пилообразную форму, что гарантирует их надежное удержание в тканях, предотвращает смещение эндопротеза относительно дефекта и позволяет отказаться от наложения швов. Наибольшая ширина лучей в местах их соединения с центральной частью обеспечивает прочность данного соединения и исключает дислокацию имплантата. Для повышения прочности всей конструкции в периферийной части полипропиленовая нить (5) прошнурована через отверстия, содержащиеся на диаметрально противоположных монолитных полосках периферийной части.Double continuous strips (3) connect the mesh and the film, forming a channel containing a polypropylene thread (5) between the mesh and the film. The peripheral part (4) in the form of monolithic strips - rays with a length of C - from 50 to 150 mm serves to fix the device in the abdominal wall during the operation. The edges of the rays have a sawtooth shape, which guarantees their reliable retention in the tissues, prevents the endoprosthesis from shifting relative to the defect and eliminates suturing. The greatest width of the rays in the places of their connection with the central part ensures the strength of this connection and eliminates the dislocation of the implant. To increase the strength of the entire structure in the peripheral part, the polypropylene yarn (5) is laced through holes contained in diametrically opposite monolithic strips of the peripheral part.
Фигура 2 - часть центральной части в разрезе.Figure 2 - part of the Central part in the context.
Центральная часть состоит из сетки (6), пленки (7) и соединяющих сетку с пленкой двойных полосок (3) толщинойThe central part consists of a grid (6), a film (7) and double strips (3) connecting the grid with a film
h - от 0,2 до 1 мм.h - from 0.2 to 1 mm.
Одна поверхность (8) пленки (7) гладкая и предназначена для контакта с органами брюшной полости. Степень шероховатости гладкого слоя от 10 до 20 нанометров, что исключает прорастание прилежащих к этому слою тканей в эндопротез в ходе эксплуатации, образование грубых рубцов и спаек со стороны органов брюшной полости. Достижение такой гладкости при обработке материала технологически сложная задача во всем мире. В случае заявленного изделия такая степень шероховатости материала легко достигается непосредственно в процессе производства. Другая поверхность пленки (7), обращенная к сетке (6), шероховатая или имеет рельефный рисунок. В случае рельефного рисунка диаметр d ячейки сетки (6) меньше диаметра D окружности, описанной вокруг образующего элемента рельефного рисунка, содержащегося на одной из поверхностей пленки. Толщина двойных полосок (3) и разница в диаметрах позволяют молодой соединительной ткани (9) обрасти вокруг полимерной части ячеек сетки (6), обеспечивая тем самым надежную окончательную фиксацию.One surface (8) of the film (7) is smooth and is intended for contact with abdominal organs. The degree of roughness of the smooth layer is from 10 to 20 nanometers, which excludes the growth of tissues adjacent to this layer into the endoprosthesis during operation, the formation of rough scars and adhesions from the abdominal organs. Achieving such smoothness when processing material is a technologically challenging task worldwide. In the case of the claimed product, this degree of roughness of the material is easily achieved directly in the production process. The other surface of the film (7), facing the grid (6), is rough or has a relief pattern. In the case of a relief pattern, the diameter d of the mesh cell (6) is smaller than the diameter D of the circle described around the forming element of the relief pattern contained on one of the surfaces of the film. The thickness of the double strips (3) and the difference in diameters allow the young connective tissue (9) to grow around the polymer part of the mesh cells (6), thereby ensuring reliable final fixation.
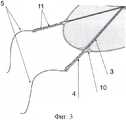
Фигура 3 - вид периферийной части эндопротеза.Figure 3 is a view of the peripheral part of the endoprosthesis.
Эндопротез изготавливается из эластичного материала, который позволяет эндопротезу принять естественную куполообразную форму брюшины без образования складок. Но, как правило, материал, который обладает хорошей эластичностью, обладает недостаточной прочностью. Высокая прочность эндопротеза особенно важна в момент протягивания лучей сквозь слои брюшины, когда создается наибольшая сила натяжения, приходящаяся на монолитные полоски (лучи) (4). Чтобы избежать разрыва последних, эндопротез укрепляют полипропиленовыми нитями. На протяжении луча (4) полипропиленовая нить прошнуровывается через отверстия (11). У основания луча (10) нить входит в канал, образованный двойными полосками (3) между сеткой и пленкой, протягивается до основания диаметрально противоположного луча, где выходит и прошнуровывается через отверстия на диаметрально противоположном луче. В момент протягивания лучей сквозь слои брюшины хирург тянет за полипропиленовые нити. Таким образом, основная сила натяжения приходится на прочные полипропиленовые нити и разрыв лучей полностью исключается.The endoprosthesis is made of an elastic material that allows the endoprosthesis to take the natural domed shape of the peritoneum without the formation of folds. But, as a rule, a material that has good elasticity has insufficient strength. The high strength of the endoprosthesis is especially important at the moment of pulling the rays through the layers of the peritoneum, when the greatest tensile force is generated per monolithic strip (rays) (4). To avoid rupture of the latter, the endoprosthesis is strengthened with polypropylene threads. Throughout the beam (4), the polypropylene thread is laced through the holes (11). At the base of the beam (10), the thread enters the channel formed by double strips (3) between the grid and the film, stretches to the base of the diametrically opposite beam, where it exits and laces through holes in the diametrically opposite beam. At the time of drawing rays through the layers of the peritoneum, the surgeon pulls on polypropylene threads. Thus, the main tensile force falls on strong polypropylene filaments and the rupture of the rays is completely eliminated.
Фигура 4 - Вид сетки и рельефного рисунка пленки.Figure 4 - View of the grid and the relief pattern of the film.
A) Образующий элемент имеет форму шестиугольника и мультиплицирован по всей поверхности таким образом, что каждая сторона шестиугольника параллельна стороне соседствующего шестиугольника.A) The forming element has the shape of a hexagon and is multiplied over the entire surface so that each side of the hexagon is parallel to the side of the adjacent hexagon.
B) Образующий элемент имеет форму треугольника и мультиплицирован по всей поверхности таким образом, что каждая сторона треугольника параллельна стороне соседствующего треугольника.B) The forming element has the shape of a triangle and is multiplied over the entire surface so that each side of the triangle is parallel to the side of the adjacent triangle.
С) Образующий элемент имеет форму прямоугольника и мультиплицирован по всей поверхности таким образом, что каждая сторона прямоугольника параллельна стороне соседствующего прямоугольника.C) The forming element has the shape of a rectangle and is multiplied over the entire surface so that each side of the rectangle is parallel to the side of the adjacent rectangle.
Заявленный эндопротез успешно внедрен в практику, что подтверждают следующие клинические примеры, демонстрирующие в сравнении результаты имплантации аналогов, прототипа и заявленного эндопротеза.The claimed endoprosthesis has been successfully put into practice, which is confirmed by the following clinical examples, which demonstrate the comparison of the results of implantation of analogues, prototype and the claimed endoprosthesis.
Клинический пример 1. Больная В., 82 л., 6 лет назад перенесла операцию по поводу ущемленной послеоперационной вентральной грыжи. Вмешательство завершено пластикой по способу inlay с применением многослойного эндопротеза из полипропилена. Обратилась в клинику в июне 2008 года. При обследовании выявлено, что рецидива грыжи нет. Имеется абсцесс передней брюшной стенки в зоне пластики. Гнойник вскрыт и дренирован, проведен курс антибиотикотерапии. Выявлено, что его дном является полипропиленовый эндопротез. Удалось купировать гнойный процесс, больная выписана. В июле 2008 вновь обратилась по поводу гнойного парапротезного свища в том же месте. Произведена санация свища, курс антибиотикотерапии, перевязки, но свищ не закрылся. На фистулографии установлено, что в зоне пластики, в области расположения эндопротеза сформировался толстокишечный свищ. Произведена обширная реконструктивная операция с удалением полипропиленового эндопротеза, участка брюшной стенки, резекция средней трети поперечноободочной кишки со свищом, трансверзотрансверзостомия, замещение образовавшегося обширного дефекта брюшной стенки полипропиленовым эндопротезом 30×30 см. Исследован удаленный во время операции препарат, при этом установлено, что эндопротез вызвал пролежень стенки ободочной кишки и образование свища. Больная поправилась, но риск осложнений и повторного образования свища остается.Clinical example 1. Patient V., 82 years old, 6 years ago underwent surgery for a restrained postoperative ventral hernia. The intervention was completed by inlay plastic surgery using a multilayer polypropylene endoprosthesis. I went to the clinic in June 2008. An examination revealed that there was no recurrence of a hernia. There is an abscess of the anterior abdominal wall in the plastic zone. The abscess is opened and drained, a course of antibiotic therapy is carried out. It was revealed that its bottom is a polypropylene endoprosthesis. I managed to stop the purulent process, the patient was discharged. In July 2008, she again appealed for a purulent para-prosthetic fistula in the same place. The fistula was sanitized, a course of antibiotic therapy, dressings, but the fistula did not close. On fistulography, it was found that in the plastic zone, in the area of the endoprosthesis, a colonic fistula was formed. An extensive reconstructive operation was performed with the removal of the polypropylene endoprosthesis, the abdominal wall section, resection of the middle third of the transverse colon with a fistula, transversotransversostomy, replacement of the resulting extensive abdominal wall defect with a polypropylene endoprosthesis of 30 × 30 cm. The drug removed during the operation was examined, and it was established that pressure sores of the colon and fistula formation. The patient recovered, but the risk of complications and re-formation of the fistula remains.
Клинический пример 2. Больной И., 75 л., в ноябре 2008 г. поступил в урологическое отделение для оперативного лечения по поводу мочекаменной болезни, пиелонефрита слева, послеоперационной левосторонней грыжи поясничной области и послеоперационной вентральной грыжи. Произведена пиелолитотомия слева, грыжесечения, пластика дефекта в области поясницы многослойным эндопротезом из полипропилена по способу inlay (эндопротез помещен в забрюшинное пространство), пластика передней брюшной стенки эндопротезом по патенту РФ №73780 (эндопротез имплантирован интраабдоминально). Послеоперационный период имел ряд особенностей. В области имплантации эндопротеза из полипропилена сформировался гнойник, через месяц - каловый свищ. Несмотря на курсы тиенама, меронема, авелокса, таваника, перевязки, трансверзостомию, свищ долго не закрывался. Выполнена трансверзостомия, через месяц после данного вмешательства свищ закрылся, в апреле 2008 г. пациент был выписан. В апреле 2009 г. вновь поступил в клинику, в зоне имплантации полипропиленового эндопротеза сформировался большой гнойник. Последний был вскрыт, при ревизии обнаружено, что дном гнойника является полипропиленовый эндопротез. Удалить его не представляется возможным из-за грубого срастания его с окружающими тканями. Дальнейший прогноз неясен, тактика лечения в настоящее время обсуждается всем коллективом клиники. В зоне пластики передней брюшной стенки эндопротезом по патенту РФ №73780 никаких осложнений не было, рецидива грыжи нет. За время наблюдения больной перенес лапаротомное вмешательство из срединного доступа, в ходе которого выявлено, что эндопротез по патенту РФ №73780 (прототип) хорошо интегрирован в ткани брюшной стенки, но не имеет никаких грубых сращений с органами брюшной полости. Доступ в брюшную полость в зоне имплантированного эндопротеза по патенту РФ №73780 (прототип) был выполнен хирургом с минимальным стажем и опытом без каких-либо технических трудностей.Clinical example 2. Patient I., 75 years old, was admitted to the urology department in November 2008 for surgical treatment for urolithiasis, pyelonephritis on the left, postoperative left-sided hernia of the lumbar region and postoperative ventral hernia. Pyelolithotomy was performed on the left side, hernia repair, plastic surgery of the defect in the lumbar region using a multilayer polypropylene endoprosthesis using the inlay method (the prosthesis was placed in the retroperitoneal space), the anterior abdominal wall plastic was used with the endoprosthesis according to RF patent No. 73780 (the implant was implanted intra-abdominally). The postoperative period had a number of features. In the area of implant implantation, an abscess formed from polypropylene, a fecal fistula a month later. Despite the courses of Tienama, Meronema, Avelox, tavanic, dressing, transversostomy, the fistula did not close for a long time. A transversostomy was performed, a month after this intervention, the fistula closed, in April 2008 the patient was discharged. In April 2009, he entered the clinic again; a large abscess formed in the zone of implantation of the polypropylene endoprosthesis. The latter was opened, during the audit it was found that the bottom of the abscess is a polypropylene endoprosthesis. It is not possible to remove it due to coarse intergrowth with surrounding tissues. The further prognosis is unclear; treatment tactics are currently being discussed by the entire clinic staff. In the area of plasticity of the anterior abdominal wall by the endoprosthesis according to the patent of the Russian Federation No. 73780 there were no complications, there was no recurrence of hernia. During the observation, the patient underwent laparotomic intervention from the mid-access, during which it was revealed that the endoprosthesis according to the patent of the Russian Federation No. 73780 (prototype) is well integrated into the tissues of the abdominal wall, but does not have any coarse adhesions with the abdominal organs. Access to the abdominal cavity in the area of the implanted prosthesis according to RF patent No. 73780 (prototype) was performed by a surgeon with minimal experience and experience without any technical difficulties.
Клинический пример 3. Больной Д., 48 л., оперирован в 2009 г. в клинике по поводу послеоперационной вентральной грыжи. В ходе выполнения интраперитонеальной имплантации эндопротезом по патенту РФ №73780 (прототип) два луча не выдержали нагрузки при их фиксации в тканях брюшной стенки и оторвались у места своего прикрепления к центральной части эндопротеза. Это потребовало выполнения комбинированной пластики (многослойной реконструкции брюшной стенки) - дополнительно имплантирован второй эндопротез (из полипропилена).Clinical example 3. Patient D., 48 years old, was operated on in 2009 in a clinic for postoperative ventral hernia. During the implementation of intraperitoneal implantation according to the patent of the Russian Federation No. 73780 (prototype), two beams could not withstand the load when they were fixed in the tissues of the abdominal wall and came off at the point of attachment to the central part of the endoprosthesis. This required the implementation of combined plastic surgery (multilayer reconstruction of the abdominal wall) - a second endoprosthesis (made of polypropylene) was additionally implanted.
Клинический пример 4. Больной С., 68 л., поступил в клинику в 2008 г. по поводу послеоперационной вентральной грыжи. Оперирован, выполнена интраабдоминальная имплантация заявленным эндопротезом. Во время имплантации никаких технических сложностей не было, отрыва фиксирующих элементов - лучей не происходило, заявленный эндопротез легко и надежно имплантирован. Послеоперационный период протекал без осложнений. Осмотрен через месяц, затем через три месяца, далее - через год. Показатели качества жизни высокие, осложнений нет, рецидива нет. На контрольном УЗИ-сканировании четко лоцируется зона пластики и заявленный эндопротез. Признаков его дислокации, рецидива грыжи нет. Петли кишечника свободно перемещаются и перистальтируют под эндопротезом. Клинических и ультрасонографических признаков образования спаек в брюшной полости нет.Clinical example 4. Patient S., 68 years old, was admitted to the clinic in 2008 for a postoperative ventral hernia. Operated, performed intra-abdominal implantation of the claimed endoprosthesis. During implantation, there were no technical difficulties, detachment of the fixing elements - rays did not occur, the claimed endoprosthesis was easily and reliably implanted. The postoperative period was uneventful. Examined after a month, then after three months, then - after a year. Quality of life indicators are high, there are no complications, no relapse. On the control ultrasound scan, the plastic zone and the claimed endoprosthesis are clearly located. There are no signs of its dislocation, hernia recurrence. Loops of the intestine move freely and peristaltize under the endoprosthesis. There are no clinical and ultrasonographic signs of adhesion formation in the abdominal cavity.
В результате анализа ближайших результатов выявлено следующее. Применение эндопротезов из пропилена по способу inlay для пластики передней брюшной стенки высокоэффективно при грыжах; у большинства пациентов метод гарантирует надежность пластики и отсутствие рецидивов, но в ряде случаев приводит к тяжелым осложнениям, требующим сложнейших реконструктивных операций. Такие наблюдения есть даже после тщательного выполнения экстраперитонизации эндопротеза. Применение заявленного эндопротеза не сопровождается опасными осложнениями, не увеличивает продолжительность лечения в стационаре и не приводит к осложнениям в ближайшем послеоперационном периоде. Материал заявленного эндопротеза исключает деформацию зоны пластики, обеспечивает надежность операции и благоприятное течение репаративного процесса. Бесшовная фиксация эндопротеза позволяет избежать формирования лигатурных абсцессов и свищей. Контакт гладкой поверхности заявленного эндопротеза с органами брюшной полости не приводит к образованию грубых спаек, пролежней стенок полых органов и формированию свищей. Другая сетчатая сторона эндопротеза надежно срастается с тканями брюшной стенки. Надежное соединение фиксирующих лучей с центральной частью эндопротеза и укрепление конструкции полипропиленовыми нитями исключает отрыв фиксирующих элементов - лучей от центральной части эндопротеза. Предлагаемый эндопротез гарантирует как надежность, так и безопасность операции.The analysis of the immediate results revealed the following. The use of propylene endoprostheses according to the inlay method for plastic surgery of the anterior abdominal wall is highly effective for hernias; in most patients, the method guarantees reliable plasticity and the absence of relapses, but in some cases leads to serious complications requiring complex reconstructive operations. Such observations are even after a thorough extraperitonization of the endoprosthesis. The use of the claimed endoprosthesis is not accompanied by dangerous complications, does not increase the duration of treatment in a hospital, and does not lead to complications in the immediate postoperative period. The material of the claimed endoprosthesis excludes deformation of the plastic zone, ensures the reliability of the operation and a favorable course of the reparative process. Seamless fixation of the endoprosthesis allows avoiding the formation of ligature abscesses and fistulas. Contact of the smooth surface of the claimed endoprosthesis with abdominal organs does not lead to the formation of coarse adhesions, pressure sores of the walls of hollow organs and the formation of fistulas. The other mesh side of the implant reliably fuses with the tissues of the abdominal wall. Reliable connection of the fixing beams with the central part of the endoprosthesis and the strengthening of the structure with polypropylene threads eliminates the separation of the fixing elements - rays from the central part of the endoprosthesis. The proposed endoprosthesis guarantees both reliability and safety of the operation.
Claims (6)
Translated fromRussianPriority Applications (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| RU2010124471/14ARU2460494C2 (en) | 2010-06-15 | 2010-06-15 | Endoprosthesis for sutureless intraabdominal plasty in case of ventral hernias |
Applications Claiming Priority (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| RU2010124471/14ARU2460494C2 (en) | 2010-06-15 | 2010-06-15 | Endoprosthesis for sutureless intraabdominal plasty in case of ventral hernias |
Publications (2)
| Publication Number | Publication Date |
|---|---|
| RU2010124471A RU2010124471A (en) | 2011-12-20 |
| RU2460494C2true RU2460494C2 (en) | 2012-09-10 |
Family
ID=45403977
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| RU2010124471/14ARU2460494C2 (en) | 2010-06-15 | 2010-06-15 | Endoprosthesis for sutureless intraabdominal plasty in case of ventral hernias |
Country Status (1)
| Country | Link |
|---|---|
| RU (1) | RU2460494C2 (en) |
Cited By (5)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2553207C2 (en)* | 2013-11-01 | 2015-06-10 | Сергей Владимирович Шалашов | Device for plasty in case of post-operative hernia of anterior abdominal wall |
| WO2015124860A1 (en)* | 2014-02-19 | 2015-08-27 | Cousin Biotech | Implantable device especially for the reconstruction of the abdominal wall |
| RU2652074C1 (en)* | 2017-02-27 | 2018-04-24 | федеральное государственное бюджетное учреждение "Центральный научно-исследовательский институт стоматологии и челюстно-лицевой хирургии" Министерства здравоохранения Российской Федерации | Mesh implant installation tool |
| RU2780937C1 (en)* | 2021-07-12 | 2022-10-04 | Общество с ограниченной ответственностью "Айкон Лаб ГмбХ" | Endoprosthesis for inguinal hernia surgery in men |
| WO2023287318A1 (en)* | 2021-07-12 | 2023-01-19 | Общество с ограниченной ответственностью "Айкон Лаб ГмбХ" | Endoprosthesis for inguinal hernia surgery |
Citations (8)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| DE19830804A1 (en)* | 1997-07-14 | 1999-05-06 | Roderick B Brown | Patch for endoscopic repair of hernias |
| US5916225A (en)* | 1994-09-29 | 1999-06-29 | Surgical Sense, Inc. | Hernia mesh patch |
| WO1999051163A1 (en)* | 1998-04-03 | 1999-10-14 | Bionx Implants Oy | Hernia mesh |
| EP1101454A1 (en)* | 1999-11-19 | 2001-05-23 | Ethicon, Inc. | A device for deploying medical textile implants |
| CN101112335A (en)* | 2006-07-28 | 2008-01-30 | 北京天助畅运医疗技术有限公司 | Embeddable multipurpose external hernia remedying slice |
| RU73780U1 (en)* | 2008-02-05 | 2008-06-10 | ООО Предприятие "Репер-НН" | GRID IMPLANT FOR ATENION PLASTIC OF THE FRONT ABDOMINAL WALL |
| RU80652U1 (en)* | 2008-09-25 | 2009-02-20 | Федеральное Государственное Учреждение "Всероссийский Центр Глазной И Пластической Хирургии Федерального Агентства По Здравоохранению И Социальному Развитию" (Фгу "Вцгпх Росздрава") | PROSTHESIS FOR SEAMLESS GERNIOPLASTY |
| RU2365342C1 (en)* | 2008-01-24 | 2009-08-27 | Государственное образовательное учреждение высшего профессионального образования Нижегородская государственная медицинская академия Росздрава (ГОУ ВПО НижГМА Роздрава) | Method of endoprosthesis bracing at performance of non-tension plasty of anterior abdominal wall |
- 2010
- 2010-06-15RURU2010124471/14Apatent/RU2460494C2/enactive
Patent Citations (8)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US5916225A (en)* | 1994-09-29 | 1999-06-29 | Surgical Sense, Inc. | Hernia mesh patch |
| DE19830804A1 (en)* | 1997-07-14 | 1999-05-06 | Roderick B Brown | Patch for endoscopic repair of hernias |
| WO1999051163A1 (en)* | 1998-04-03 | 1999-10-14 | Bionx Implants Oy | Hernia mesh |
| EP1101454A1 (en)* | 1999-11-19 | 2001-05-23 | Ethicon, Inc. | A device for deploying medical textile implants |
| CN101112335A (en)* | 2006-07-28 | 2008-01-30 | 北京天助畅运医疗技术有限公司 | Embeddable multipurpose external hernia remedying slice |
| RU2365342C1 (en)* | 2008-01-24 | 2009-08-27 | Государственное образовательное учреждение высшего профессионального образования Нижегородская государственная медицинская академия Росздрава (ГОУ ВПО НижГМА Роздрава) | Method of endoprosthesis bracing at performance of non-tension plasty of anterior abdominal wall |
| RU73780U1 (en)* | 2008-02-05 | 2008-06-10 | ООО Предприятие "Репер-НН" | GRID IMPLANT FOR ATENION PLASTIC OF THE FRONT ABDOMINAL WALL |
| RU80652U1 (en)* | 2008-09-25 | 2009-02-20 | Федеральное Государственное Учреждение "Всероссийский Центр Глазной И Пластической Хирургии Федерального Агентства По Здравоохранению И Социальному Развитию" (Фгу "Вцгпх Росздрава") | PROSTHESIS FOR SEAMLESS GERNIOPLASTY |
Cited By (6)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2553207C2 (en)* | 2013-11-01 | 2015-06-10 | Сергей Владимирович Шалашов | Device for plasty in case of post-operative hernia of anterior abdominal wall |
| WO2015124860A1 (en)* | 2014-02-19 | 2015-08-27 | Cousin Biotech | Implantable device especially for the reconstruction of the abdominal wall |
| US10632233B2 (en) | 2014-02-19 | 2020-04-28 | Cousin Biotech | Implantable device, especially for the reconstruction of the abdominal wall |
| RU2652074C1 (en)* | 2017-02-27 | 2018-04-24 | федеральное государственное бюджетное учреждение "Центральный научно-исследовательский институт стоматологии и челюстно-лицевой хирургии" Министерства здравоохранения Российской Федерации | Mesh implant installation tool |
| RU2780937C1 (en)* | 2021-07-12 | 2022-10-04 | Общество с ограниченной ответственностью "Айкон Лаб ГмбХ" | Endoprosthesis for inguinal hernia surgery in men |
| WO2023287318A1 (en)* | 2021-07-12 | 2023-01-19 | Общество с ограниченной ответственностью "Айкон Лаб ГмбХ" | Endoprosthesis for inguinal hernia surgery |
Also Published As
| Publication number | Publication date |
|---|---|
| RU2010124471A (en) | 2011-12-20 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| Bendavid | Composite mesh (polypropylene-e-PTFE) in the intraperitoneal position: a report of 30 cases | |
| KR20180102083A (en) | Light letters and medical materials | |
| RU2524196C1 (en) | Reinforced warp mesh endoprosthesis for ventral hernia repair (versions) and method for using it | |
| EP1079762A1 (en) | Hernia mesh | |
| RU121735U1 (en) | GRID IMPLANT FOR RECONSTRUCTIVE SURGERY (OPTIONS) | |
| RU2460494C2 (en) | Endoprosthesis for sutureless intraabdominal plasty in case of ventral hernias | |
| Klobusicky et al. | Reduction of chronic post-herniotomy pain and recurrence rate. Use of the anatomical self-gripping ProGrip laparoscopic mesh in TAPP hernia repair. Preliminary results of a prospective study | |
| Ikada | Bioabsorbable fibers for medical use | |
| RU2503430C1 (en) | Endoprosthesis for treating paracolostomal hernias | |
| RU2524308C1 (en) | Reinforced warp mesh endoprosthesis for inguinal hernia repair (versions) and method for using it | |
| RU73780U1 (en) | GRID IMPLANT FOR ATENION PLASTIC OF THE FRONT ABDOMINAL WALL | |
| Pandit et al. | Design of surgical meshes–an engineering perspective | |
| RU2381770C2 (en) | Herniosystem for atension hernia repair | |
| RU2519638C2 (en) | Multipurpose endoprosthesis for abdominoplasty (versions) | |
| Simmermacher et al. | Biomaterials for abdominal wall reconstruction | |
| Kang et al. | Suture Techniques and Selection | |
| RU89374U1 (en) | IMPLANT FOR PLASTIC DEFECTS OF THE SOLID BRAIN Shell | |
| RU2784168C1 (en) | Endoprosthesis for surgical treatment of parastomal hernias using the ipom technique | |
| Peniston et al. | Design of abdominal wall hernioplasty meshes guided by mechanobiology and the wound healing response | |
| RU166460U1 (en) | Mesh implant for prolapse and urinary stress incontinence | |
| US12285346B2 (en) | Thin-film micromesh and related methods | |
| RU2605688C2 (en) | Method of prosthetic reconstructive preperitoneal hernioplasty for exomphalos and epigastric hernias | |
| RU2423933C1 (en) | Method of hernial defect plasty in case of large ventral hernias | |
| RU2780937C1 (en) | Endoprosthesis for inguinal hernia surgery in men | |
| Zgheib et al. | Migration of an abdominal mesh into a reconstructed ileal neobladder, diagnosis and management: A case report |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| PC41 | Official registration of the transfer of exclusive right | Effective date:20140520 |