RU2371120C1 - Oesophageal enteroanastomosis technique - Google Patents
Oesophageal enteroanastomosis techniqueDownload PDFInfo
- Publication number
- RU2371120C1 RU2371120C1RU2008133697/14ARU2008133697ARU2371120C1RU 2371120 C1RU2371120 C1RU 2371120C1RU 2008133697/14 ARU2008133697/14 ARU 2008133697/14ARU 2008133697 ARU2008133697 ARU 2008133697ARU 2371120 C1RU2371120 C1RU 2371120C1
- Authority
- RU
- Russia
- Prior art keywords
- anastomosis
- oesophagus
- loop
- intestinal
- small intestine
- Prior art date
Links
- 238000000034methodMethods0.000titleclaimsabstractdescription14
- 230000003872anastomosisEffects0.000claimsabstractdescription23
- 210000000813small intestineAnatomy0.000claimsabstractdescription13
- 230000000968intestinal effectEffects0.000claimsabstractdescription10
- 210000000936intestineAnatomy0.000claimsabstractdescription6
- 230000015572biosynthetic processEffects0.000claimsabstractdescription5
- 210000003238esophagusAnatomy0.000claimsdescription15
- 238000013459approachMethods0.000claimsdescription2
- 238000007599dischargingMethods0.000claims1
- 239000003814drugSubstances0.000abstractdescription3
- 238000001356surgical procedureMethods0.000abstractdescription3
- 206010028980NeoplasmDiseases0.000abstractdescription2
- 201000011510cancerDiseases0.000abstractdescription2
- 210000002784stomachAnatomy0.000abstractdescription2
- 230000000694effectsEffects0.000abstract1
- 239000000126substanceSubstances0.000abstract1
- 208000005718Stomach NeoplasmsDiseases0.000description3
- 210000001519tissueAnatomy0.000description3
- 238000002224dissectionMethods0.000description2
- 238000013110gastrectomyMethods0.000description2
- 210000001165lymph nodeAnatomy0.000description2
- 201000000498stomach carcinomaDiseases0.000description2
- 206010027476MetastasesDiseases0.000description1
- 239000008280bloodSubstances0.000description1
- 210000004369bloodAnatomy0.000description1
- 206010017758gastric cancerDiseases0.000description1
- 210000001035gastrointestinal tractAnatomy0.000description1
- 238000007654immersionMethods0.000description1
- 238000002350laparotomyMethods0.000description1
- 238000012544monitoring processMethods0.000description1
- 230000002980postoperative effectEffects0.000description1
- 201000011549stomach cancerDiseases0.000description1
- 230000007704transitionEffects0.000description1
- 230000029663wound healingEffects0.000description1
Images


Landscapes
- Medicines That Contain Protein Lipid Enzymes And Other Medicines (AREA)
Abstract
Description
Translated fromRussianИзобретение относится к области медицины, а именно - онкологии.The invention relates to medicine, namely to Oncology.
Известны и широко используются различные способы анастомозирования пищевода и тонкой кишки [2]. Существуют различные подходы к анастомозированию этих отделов пищеварительного тракта: инвагинационные, погружные анастомозы, анастомозы, предусматривающие окутывание линии пищеводно-кишечного шва приводящей, отводящей или обеими петлями тонкой кишки. Принцип создания последней из упомянутых разновидностей пищеводно-кишечных анастомозов один - защита линии швов кишечной стенкой. Но реализуется он различными путями. На наш взгляд, основные различия всех подобных анастомозов в удобстве их формирования, что определяется количеством и сложностью швов, необходимых для его формирования, и в надежности, что обусловлено полнотой окутывания. Все ранее предложенные способы подобных анастомозов отличались тем, что удачное решение одного из вышеупомянутых условий решалось за счет другого. Яркими примерами в этом отношении являются анастомоз по Гиляровичу [2] и анастомоз по Бондарю [1]. Первый из которых прост и быстр в формировании, но при этом не всегда удается создать достаточный избыток тканей для надежного укрытия кишечной стенкой линии пищеводно-кишечного анастомоза. Второй позволяет надежно укрыть линию анастомоза, но требует наложения значительно большего количества швов.Various methods of anastomosing the esophagus and small intestine are known and widely used [2]. There are various approaches to the anastomosis of these sections of the digestive tract: invagination, immersion anastomoses, anastomoses, providing for enveloping the line of the esophageal-intestinal suture of the adducting, abducting, or both loops of the small intestine. The principle of creating the last of the mentioned types of esophageal-intestinal anastomoses is one - the protection of the suture line of the intestinal wall. But it is implemented in various ways. In our opinion, the main differences of all such anastomoses in the convenience of their formation, which is determined by the number and complexity of the joints necessary for its formation, and in reliability, due to the completeness of enveloping. All previously proposed methods for such anastomoses were distinguished in that a successful solution to one of the above conditions was decided at the expense of the other. Vivid examples in this regard are the anastomosis according to Gilyarovich [2] and the anastomosis according to Bondar [1]. The first of which is simple and quick to form, but it is not always possible to create a sufficient excess of tissues to reliably cover the intestinal wall of the line of the esophageal-intestinal anastomosis. The second allows you to reliably cover the line of the anastomosis, but requires the application of a significantly larger number of sutures.
Для устранения ограничений вышеуказанных способов анастомозирования пищевода и тонкой кишки нами предложен новый способ эзофаго-энтероанастомоза.To eliminate the limitations of the above methods for anastomosing the esophagus and small intestine, we proposed a new method of esophago-enteroanastomosis.
Цель изобретения - улучшение результатов хирургического лечения рака желудка и дистального отдела пищевода путем использования оригинального способа эзофаго-энтероанастомоза.The purpose of the invention is the improvement of the results of surgical treatment of cancer of the stomach and the distal esophagus by using the original method of esophago-enteroanastomosis.
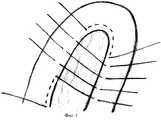
Предложенный способ эзофаго-энтероанастомоза осуществляется следующим образом. На фиг.1 в 50-ти см от дуоденоеюнального перехода четырьмя - пятью широкими продольными стежками вдоль брыжеечнного края прошивается тонкая кишка. Нить завязывается, формируя, таким образом, верхушку кишечной петли (при этом создается избыток тканей для укутывания анастомоза с одной стороны). Ниже, в описании, кишка, находящаяся проксимальнее этого шва, будет называться приводящей, а дистальнее - отводящей. Далее тремя лигатурам, отступя 0,6-0,7 см друг от друга сшиваются брыжеечные края приводящей и отводящей кишки. Этими же нитями прошивается задняя стенка пересеченного пищевода в 0,7 см от пищеводного зажима, после чего они берутся на держалки без завязывания. Отступя 0,7 см от последней лигатуры прошивается брыжеечный край отводящей и приводящей петли и далее, этой же нитью, четырьмя - пятью широкими продольными стежками вдоль брыжеечнного края, в проксимальном направлении прошивается приводящая кишка и завязывается (тем самым формируется избыток тканей для укутывания анастомоза с другой стороны). Затем (на фиг.2) перпендикулярно наложенным швам на переднюю стенку приводящей кишки (на уровне первой и третьей не завязанных лигатур) и на заднюю стенку пищевода накладываются и поочередно завязываются по два шва на расстоянии 0,5-0,7 см друг от друга. После чего завязываются и предварительно наложенные лигатуры. Затем, после циркулярного пересечения пищевода под зажимом и рассечения отводящей петли тонкой кишки продольно, формируется пищеводно-кишечный шов отдельными лигатурами путем вшивания пересеченного пищевода в разрез тонкой кишки. Затем отдельными лигатурами укрывается передняя стенка анастомоза путем сшивания над ним и дистальным отрезком пищевода тонкой кишки, подхватываемой из зоны ранее сформированных избытков справа и слева от пищевода (фиг.3).The proposed method esophago-enteroanastomosis is as follows. In FIG. 1, a small intestine is stitched with four to five wide longitudinal stitches along the mesenteric edge 50 cm from the duodenojejunal junction. The thread is tied, thus forming the tip of the intestinal loop (this creates an excess of tissue to wrap the anastomosis on one side). Below, in the description, the intestine located proximal to this suture will be called adducting, and distal - abduction. Then, with three ligatures, departing 0.6-0.7 cm from each other, the mesenteric edges of the adducting and abducting intestines are sutured. With the same threads, the back wall of the crossed esophagus is stitched 0.7 cm from the esophageal clamp, after which they are taken onto the holders without tying. 0.7 cm away from the last ligature, the mesenteric edge of the outlet and adduction loops is sutured and then, with the same thread, four - five wide longitudinal stitches along the mesenteric edge, the adducting intestine is stitched in the proximal direction and tied (thereby forming excess tissue to wrap the anastomosis with other side). Then (in Fig. 2), perpendicular to the sutures on the front wall of the adducting intestine (at the level of the first and third ligatures not tied) and on the back wall of the esophagus are superimposed and alternately tied two sutures at a distance of 0.5-0.7 cm from each other . After that, previously imposed ligatures are tied. Then, after a circular intersection of the esophagus under the clamp and dissection of the outlet loop of the small intestine longitudinally, an esophageal-intestinal suture is formed by separate ligatures by suturing the crossed esophagus into the incision of the small intestine. Then, the anastomosis anterior wall is covered by separate ligatures by stitching above it and the distal segment of the esophagus of the small intestine, taken from the zone of previously formed excesses to the right and left of the esophagus (Fig. 3).
Данный способ эзофаго-энтероанастомоза облегчает и ускоряет выполнение операции, обеспечивая при этом ее максимальную надежность.This method of esophago-enteroanastomosis facilitates and accelerates the operation, while ensuring its maximum reliability.
Описанный способ применен у пятнадцати пациентов как реконструктивный этап при выполнении гастрэктомий по поводу рака желудка.The described method was used in fifteen patients as a reconstructive step in the performance of gastrectomy for gastric cancer.
Клинический пример: Больной И., 1952 г.р., оперирован в 1-м хирургическом отделении РОКОД 25.04.06. По поводу рака верхней трети тела желудка T3N1MO выполнена расширенная гастрэктомия с лимфодиссекцией Д2. Эзофаго-энтероанастомоз сформирован по оригинальной методике. Продолжительность оперативного вмешательства 2 часа 45 минут, кровопотеря 250 мл. Гистология №9182-200: недифференцированный рак желудка с переходом на пищевод, прорастает все слои, метастазы в 2 лимфатических узла малой кривизны. Гладкое течение послеоперационного периода. На 6-е сутки рентгенологический контроль состояния анастомоза - анастомоз состоятелен. Заживление лапаротомной раны первичным натяжением. Выписан на 11-е суткиClinical example: Patient I., born in 1952, operated on in the 1st surgical department of the ROKOD on 04.25.06. For cancer of the upper third of the T3N1MO stomach, an extended gastrectomy with lymph node dissection D2 was performed. Esophago-enteroanastomosis is formed according to the original method. Duration of surgery 2 hours 45 minutes, blood loss 250 ml. Histology No. 9182-200: undifferentiated cancer of the stomach with a transition to the esophagus, all layers germinate, metastases in 2 lymph nodes of lesser curvature. Smooth postoperative period. On the 6th day, radiological monitoring of the state of the anastomosis - the anastomosis is consistent. Laparotomy wound healing by primary intention. Discharged on the 11th day
Клиническая апробация способа показала его эффективность в плане удобства, быстроты формирования и надежности (случаев несостоятельности анастомоза не отмечено).Clinical testing of the method showed its effectiveness in terms of convenience, speed of formation and reliability (cases of insolvency of the anastomosis were not noted).
Источники информацииInformation sources
1. Клименков А.А. Опухоли желудка. - М.: Медицина, 1988.1. Klimenkov A.A. Tumors of the stomach. - M .: Medicine, 1988.
2. Шалимов А.А., Саенко В.Ф. Хирургия пищеварительного тракта. - Киев: Здоровь̀я, 1987. - 586 с.2. Shalimov A.A., Saenko V.F. Digestive tract surgery. - Kiev: Health, 1987. - 586 p.
Claims (1)
Translated fromRussianPriority Applications (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| RU2008133697/14ARU2371120C1 (en) | 2008-08-15 | 2008-08-15 | Oesophageal enteroanastomosis technique |
Applications Claiming Priority (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| RU2008133697/14ARU2371120C1 (en) | 2008-08-15 | 2008-08-15 | Oesophageal enteroanastomosis technique |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| RU2371120C1true RU2371120C1 (en) | 2009-10-27 |
Family
ID=41352968
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| RU2008133697/14ARU2371120C1 (en) | 2008-08-15 | 2008-08-15 | Oesophageal enteroanastomosis technique |
Country Status (1)
| Country | Link |
|---|---|
| RU (1) | RU2371120C1 (en) |
Citations (5)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US4964863A (en)* | 1987-06-10 | 1990-10-23 | Moskovsky Gorodskoi Nauchno-Issledovatelsky Institut Skoroi Pomoschi Imeni N.V. Sklifosovskogo | Device for establishing esophagoenterostomies |
| RU2002116891A (en)* | 2002-06-24 | 2004-02-10 | Волгоградска медицинска академи | The method of formation of esophagoenteroanastomosis in conditions of lack of plastic material |
| RU2234253C2 (en)* | 2002-03-25 | 2004-08-20 | Сергеев Иван Васильевич | Method for applying esophagojejunoanastomosis at gastrectomy |
| RU2248759C2 (en)* | 2003-05-29 | 2005-03-27 | Павловская центральная районная больница Нижегородской области | Method for esophagojejunoanastomosis at gastrectomy |
| UA33952U (en)* | 2008-01-02 | 2008-07-25 | Одесский Государственный Медицинский Университет | Technique for invagination mode of applying esophageal-intestinal anastomosis |
- 2008
- 2008-08-15RURU2008133697/14Apatent/RU2371120C1/ennot_activeIP Right Cessation
Patent Citations (5)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US4964863A (en)* | 1987-06-10 | 1990-10-23 | Moskovsky Gorodskoi Nauchno-Issledovatelsky Institut Skoroi Pomoschi Imeni N.V. Sklifosovskogo | Device for establishing esophagoenterostomies |
| RU2234253C2 (en)* | 2002-03-25 | 2004-08-20 | Сергеев Иван Васильевич | Method for applying esophagojejunoanastomosis at gastrectomy |
| RU2002116891A (en)* | 2002-06-24 | 2004-02-10 | Волгоградска медицинска академи | The method of formation of esophagoenteroanastomosis in conditions of lack of plastic material |
| RU2248759C2 (en)* | 2003-05-29 | 2005-03-27 | Павловская центральная районная больница Нижегородской области | Method for esophagojejunoanastomosis at gastrectomy |
| UA33952U (en)* | 2008-01-02 | 2008-07-25 | Одесский Государственный Медицинский Университет | Technique for invagination mode of applying esophageal-intestinal anastomosis |
Non-Patent Citations (2)
| Title |
|---|
| SCHREIBER HW et al., Esophagojejunostomy anastomosis technique, Langenbecks Arch Chir, 1975 Jun 9; 338(3):159-67, (реферат), [он-лайн], [найдено 28.02.2009], найдено из базы данных Pubmed.* |
| ШАЛИМОВ А.А., САЕНКО В.Ф. Хирургия пищеварительного тракта, 1987, с.273-279.* |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| Edwards | Resection and anastomosis of small intestine: current methods applicable to the horse | |
| RU2202293C2 (en) | Method for applying intestinal suture | |
| RU2371120C1 (en) | Oesophageal enteroanastomosis technique | |
| RU2364352C1 (en) | Suturing technique applied in formation of oesophagogastric anastomosis | |
| RU2401076C1 (en) | Oesophagogastric anastomosis technique | |
| RU2328992C1 (en) | Method of surgical formation of invaginated one-row large intestinal anastomosis | |
| RU2293530C1 (en) | Method for forming terminolateral pancreatojejunoanastomosis at pancreatoduodenal resection | |
| RU2452412C2 (en) | Method of esophagointestinal anastomosis | |
| RU2155539C2 (en) | Method for applying gastrectomy | |
| RU2221502C1 (en) | Method for forming compression-valvular choledochoenteroanastomosis | |
| RU2826391C1 (en) | Gastro-oesophageal anastomosis formation method | |
| RU2645116C2 (en) | Method for laparoscopic intracorporal manual gastroenteroanastomosis | |
| RU2535075C2 (en) | Method of forming end-side oesophageal-gastric anastomosis after proximal stomach resection | |
| RU2328229C1 (en) | Method of similar intestinal continuity restoration | |
| RU2296518C1 (en) | Method for forming compression-valvular esophageal-small-intestinal anastomosis | |
| RU2657938C1 (en) | Method of application of an intestinal suture | |
| RU2180192C2 (en) | Method for carrying out esophagojejunostomy when performing gastrectomy and esophagectomy | |
| RU2456943C1 (en) | Method of applying anastomosis between hollow organs of abdominal cavity | |
| RU2197903C2 (en) | Method for gastroduodenoanastomosis | |
| RU2221496C2 (en) | Method for surgical treating pyloroduodenal ulcers complicated with stenosis of output gastric department | |
| RU2209599C2 (en) | Method for subtotal proximal resection of stomach | |
| SU1694119A1 (en) | Method for forming the terminal intestinal anastomosis | |
| RU2327426C1 (en) | Method of areflux oesophageal-intestinal anastomosis formation following gastrectomy | |
| RU2207069C2 (en) | Method for developing areflux cervical esophageal-large intestinal anastomosis | |
| RU2290877C1 (en) | Method for reconstructing circulation in portal vein system after pancreatoduodenal resection |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| MM4A | The patent is invalid due to non-payment of fees | Effective date:20100816 |