RU2371106C1 - Inguinal hernia repair technique - Google Patents
Inguinal hernia repair techniqueDownload PDFInfo
- Publication number
- RU2371106C1 RU2371106C1RU2008114794/14ARU2008114794ARU2371106C1RU 2371106 C1RU2371106 C1RU 2371106C1RU 2008114794/14 ARU2008114794/14 ARU 2008114794/14ARU 2008114794 ARU2008114794 ARU 2008114794ARU 2371106 C1RU2371106 C1RU 2371106C1
- Authority
- RU
- Russia
- Prior art keywords
- aponeurosis
- mesh prosthesis
- inguinal
- oblique muscle
- muscle
- Prior art date
Links
- 238000000034methodMethods0.000titleclaimsabstractdescription26
- 208000029836Inguinal HerniaDiseases0.000titleclaimsdescription14
- 230000008439repair processEffects0.000titleabstractdescription3
- 210000003205muscleAnatomy0.000claimsabstractdescription43
- 210000004267spermatic cordAnatomy0.000claimsabstractdescription28
- 210000003041ligamentAnatomy0.000claimsabstractdescription19
- 238000002224dissectionMethods0.000claimsabstractdescription6
- 210000001015abdomenAnatomy0.000claimsdescription25
- 238000002316cosmetic surgeryMethods0.000claimsdescription6
- 238000002955isolationMethods0.000claimsdescription4
- 238000012545processingMethods0.000claimsdescription4
- 210000005036nerveAnatomy0.000abstractdescription11
- 230000002980postoperative effectEffects0.000abstractdescription6
- 206010019909HerniaDiseases0.000abstractdescription4
- 239000003814drugSubstances0.000abstractdescription3
- 230000015572biosynthetic processEffects0.000abstractdescription2
- 230000003187abdominal effectEffects0.000abstract5
- 230000000694effectsEffects0.000abstract1
- 230000008030eliminationEffects0.000abstract1
- 238000003379elimination reactionMethods0.000abstract1
- 239000000126substanceSubstances0.000abstract1
- 210000000494inguinal canalAnatomy0.000description15
- 239000004743PolypropyleneSubstances0.000description11
- -1polypropylenePolymers0.000description11
- 229920001155polypropylenePolymers0.000description11
- 238000001356surgical procedureMethods0.000description7
- 210000003195fasciaAnatomy0.000description4
- 208000024891symptomDiseases0.000description4
- 210000003815abdominal wallAnatomy0.000description3
- 239000007943implantSubstances0.000description3
- 210000000564inguinal ringAnatomy0.000description3
- 210000000545internal inguinal ringAnatomy0.000description3
- 206010033675panniculitisDiseases0.000description3
- 239000004033plasticSubstances0.000description3
- 210000003689pubic boneAnatomy0.000description3
- 210000004304subcutaneous tissueAnatomy0.000description3
- 238000011477surgical interventionMethods0.000description3
- 206010021620Incisional herniasDiseases0.000description2
- 239000004792ProleneSubstances0.000description2
- 206010052428WoundDiseases0.000description2
- 208000027418Wounds and injuryDiseases0.000description2
- 210000000683abdominal cavityAnatomy0.000description2
- 210000003489abdominal muscleAnatomy0.000description2
- 210000003484anatomyAnatomy0.000description2
- 230000008901benefitEffects0.000description2
- 238000011835investigationMethods0.000description2
- 239000000463materialSubstances0.000description2
- 210000001139rectus abdominisAnatomy0.000description2
- 210000001519tissueAnatomy0.000description2
- 210000001215vaginaAnatomy0.000description2
- 241000766026Coregonus nasusSpecies0.000description1
- 206010053692Wound complicationDiseases0.000description1
- 229940035676analgesicsDrugs0.000description1
- 239000000730antalgic agentSubstances0.000description1
- 230000008859changeEffects0.000description1
- 238000010835comparative analysisMethods0.000description1
- 230000006835compressionEffects0.000description1
- 238000007906compressionMethods0.000description1
- 238000011161developmentMethods0.000description1
- 230000007717exclusionEffects0.000description1
- 230000003993interactionEffects0.000description1
- 238000012986modificationMethods0.000description1
- 230000004048modificationEffects0.000description1
- 230000037023motor activityEffects0.000description1
- 230000003533narcotic effectEffects0.000description1
- RJMUSRYZPJIFPJ-UHFFFAOYSA-NniclosamideChemical compoundOC1=CC=C(Cl)C=C1C(=O)NC1=CC=C([N+]([O-])=O)C=C1ClRJMUSRYZPJIFPJ-UHFFFAOYSA-N0.000description1
- 210000000505parietal peritoneumAnatomy0.000description1
- 238000002360preparation methodMethods0.000description1
- 230000008569processEffects0.000description1
- 230000009467reductionEffects0.000description1
- 238000002271resectionMethods0.000description1
- 210000000546superficial inguinal ringAnatomy0.000description1
- 239000003356suture materialSubstances0.000description1
- 208000011580syndromic diseaseDiseases0.000description1
- 210000002435tendonAnatomy0.000description1
- 210000001550testisAnatomy0.000description1
- 238000011144upstream manufacturingMethods0.000description1
- 230000002792vascularEffects0.000description1
- 230000000007visual effectEffects0.000description1
Images

Landscapes
- Prostheses (AREA)
Abstract
Description
Translated fromRussianИзобретение относится к области медицины, а именно к герниологии, и предназначено для снижения болевого синдрома после операции при паховой грыже.The invention relates to medicine, namely to herniology, and is intended to reduce pain after surgery for inguinal hernia.
Известен способ паховой герниопластики по Лихтенштейну, который предусматривает выполнение традиционного переднего доступа к паховому каналу и пластику его задней стенки полипропиленовой сеткой. После вскрытия пахового канала выделяют паховую связку, семенной канатик, выделяют и обрабатывают грыжевой мешок. Полипропиленовую сетку моделируют по форме пахового канала и фиксируют непрерывным швом к паховой связке до внутреннего пахового кольца. В медиальной части раны сетка должна перекрывать лонную кость на 1,5-2 см. Отдельными швами нерассасывающимся материалом сетку фиксируют к внутренней косой мышце. Латеральный край сетки рассекают на 2 части: 2/3 выше и 1/3 ниже семенного канатика. Верхнюю браншу захватывают, протягивают над семенным канатиком и отдельными швами фиксируют к паховой связке (Чижов Д.В., Шурыгин С.Н., Воскресенский П.К., Филаткина Н.В. Пластика пахового канала по Лихтенштейну и ее модификации. - Герниология, 2004, №1, с.43-51). Апоневроз наружной косой мышцы при пластике по Лихтенштейну сшивают край в край без натяжения. Диаметр формирующегося наружного пахового кольца в данном случае не имеет значения. После этого рану зашивают обычным образом (Тимошин А.Д., Юрасов А.В., Шестаков А.Л. Хирургическое лечение паховых и послеоперационных грыж брюшной стенки. М.: Триада-X, 2003, с.25-27).A known method of inguinal hernioplasty according to Liechtenstein, which provides for the implementation of traditional front access to the inguinal canal and the plastic of its posterior wall with a polypropylene mesh. After opening the inguinal canal, the inguinal ligament and spermatic cord are isolated, the hernial sac is isolated and treated. The polypropylene mesh is modeled on the shape of the inguinal canal and fixed with a continuous suture to the inguinal ligament to the inner inguinal ring. In the medial part of the wound, the mesh should overlap the pubic bone by 1.5-2 cm. With separate seams of non-absorbable material, the mesh is fixed to the internal oblique muscle. The lateral edge of the mesh is dissected into 2 parts: 2/3 above and 1/3 below the spermatic cord. The upper jaw is grabbed, stretched over the spermatic cord and fixed to the inguinal ligament with separate sutures (Chizhov D.V., Shurygin S.N., Voskresensky P.K., Filatkina N.V. Plastic surgery of the inguinal canal according to Liechtenstein and its modifications. - Herniology , 2004, No. 1, p. 43-51). Aponeurosis of the external oblique muscle with plastic surgery according to Liechtenstein sew edge to edge without tension. The diameter of the forming external inguinal ring in this case does not matter. After this, the wound is sutured in the usual way (Timoshin A.D., Yurasov A.V., Shestakov A.L. Surgical treatment of inguinal and postoperative hernias of the abdominal wall. M: Triada-X, 2003, p.25-27).
Указанный способ герниопластики позволяет надежно укрепить заднюю стенку пахового канала. Автор на большом материале демонстрирует прекрасные результаты - 0,2% рецидивов при минимуме раневых осложнений. Техническая простота методики делает ее доступной широкому кругу хирургов.The specified method of hernioplasty allows you to reliably strengthen the back wall of the inguinal canal. The author on great material demonstrates excellent results - 0.2% of relapses with a minimum of wound complications. The technical simplicity of the technique makes it accessible to a wide range of surgeons.
Однако и этот известный способ имеет свои недостатки.However, this known method has its drawbacks.
Операция подразумевает наложение швов в зоне расположения подвздошно-подчревного и подвздошно-пахового нервов и их ветвей при фиксации верхнего края сетчатого протеза. Вышеуказанные нервы не всегда интраоперационно удается идентифицировать и поэтому сохраняется риск их захвата в лигатуры. Чаще это бывает у полных пациентов и при выраженном рубцовом процессе в паховом канале. Использование одиночных швов несколько снижает вероятность попадания подвздошно-подчревного и подвздошно-пахового нервов в лигатуры, но не исключает ее полностью. Сдавление нервов или их ветвей лигатурами в послеоперационном периоде вызывает выраженный болевой синдром в зоне оперативного вмешательства.The operation involves suturing in the area of the ileo-hypogastric and iliac-inguinal nerves and their branches during fixation of the upper edge of the mesh prosthesis. The above nerves are not always identifiable intraoperatively and therefore the risk of their capture in the ligatures remains. More often this happens in full patients and with a pronounced cicatricial process in the inguinal canal. The use of single sutures somewhat reduces the likelihood of the ileo-hypogastric and iliac-inguinal nerves getting into the ligatures, but does not completely exclude it. Compression of nerves or their branches by ligatures in the postoperative period causes severe pain in the area of surgical intervention.
Развитие принципов методики Лихтенштейна воплотилось в разработанном фирмой «Ethicon» протезе, получившем название Prolene Hernia System (PHS). Эндопротез представляет собой две пластины (лепестка) полипропиленовой сетки, соединенные полипропиленовым цилиндром. Операцию выполняют через прямой паховый доступ. Мобилизуют семенной канатик, пересекают до внутреннего пахового кольца мышцу, поднимающую яичко. Выполняют выделение и обработку грыжевого мешка. После этого между поперечной фасцией и париетальной брюшиной в сформированное пространство размещают задний (круглый) лепесток протеза PHS. Передний (овальный) лепесток конструкции ориентируют так, чтобы его длинная сторона была параллельна паховой связке. Приступают к фиксации переднего лепестка. Он должен, как при методике Лихтенштейна, наслаиваться на 1-1,5 см на влагалище прямой мышцы живота и лонный бугорок. Полипропиленовыми одиночными швами выполняют фиксацию переднего лепестка к влагалищу прямой мышцы живота, лонному бугорку, паховой связке. При косых паховых грыжах на уровне внутреннего пахового кольца рассекают нижний край переднего лепестка в направлении соединяющего цилиндра для размещения семенного канатика. При прямых паховых грыжах рассечение выполняют от наружного края переднего лепестка. Полученные в результате разреза бранши протеза сшивают вокруг семенного канатика и фиксируют к паховой связке. Дополнительными швами латеральную часть лепестка также подшивают к паховой связке. Верхний край сетки фиксируют 2-3 отдельными швами к внутренней косой мышце. Латеральную часть переднего лепестка заправляют под апоневроз наружной косой мышцы живота, который ушивают непрерывным швом (Тимошин А.Д., Юрасов А.В., Шестаков А.Л. Хирургическое лечение паховых и послеоперационных грыж брюшной стенки. М.: Триада-Х, 2003, с.27-30).The development of the principles of the Liechtenstein technique was embodied in the prosthesis developed by Ethicon, called the Prolene Hernia System (PHS). An endoprosthesis is two plates (lobes) of a polypropylene mesh connected by a polypropylene cylinder. The operation is performed through direct inguinal access. The spermatic cord is mobilized, the muscle raising the testicle is crossed to the inner inguinal ring. Isolation and processing of the hernial sac is performed. After that, between the transverse fascia and the parietal peritoneum, the back (round) lobe of the PHS prosthesis is placed in the formed space. The anterior (oval) lobe of the structure is oriented so that its long side is parallel to the inguinal ligament. Proceed to fixation of the front lobe. It should, as in the Liechtenstein technique, be layered 1-1.5 cm on the vagina of the rectus abdominis muscle and pubic tubercle. Single polypropylene sutures fix the anterior lobe to the vagina of the rectus abdominis muscle, pubic tubercle, inguinal ligament. With oblique inguinal hernias at the level of the internal inguinal ring, the lower edge of the anterior lobe is cut in the direction of the connecting cylinder to accommodate the spermatic cord. With direct inguinal hernias, dissection is performed from the outer edge of the anterior lobe. The branches of the prosthesis resulting from the incision are sutured around the spermatic cord and fixed to the inguinal ligament. With additional sutures, the lateral part of the petal is also sutured to the inguinal ligament. The upper edge of the mesh is fixed with 2-3 separate sutures to the internal oblique muscle. The lateral part of the anterior lobe is inserted under the aponeurosis of the external oblique muscle of the abdomen, which is sutured with a continuous suture (Timoshin A.D., Yurasov A.V., Shestakov A.L. Surgical treatment of inguinal and postoperative hernias of the abdominal wall. M .: Triada-X, 2003, p. 27-30).
Методика повышает надежность пластики при паховых грыжах. При этом небольшое количество одиночных швов для фиксации протеза снижает вероятность захвата в лигатуры подвздошно-подчревного и подвздошно-пахового нервов или их ветвей. Однако расположение одного из лепестков конструкции PHS в предбрюшинном пространстве усложняет вмешательство. Приходится формировать ложе в сосудистой зоне.The technique improves the reliability of plastic with inguinal hernias. At the same time, a small number of single sutures for fixing the prosthesis reduces the likelihood of capture into the ligatures of the ileo-hypogastric and iliac-inguinal nerves or their branches. However, the location of one of the lobes of the PHS construct in the preperitoneal space complicates the intervention. It is necessary to form a bed in the vascular zone.
Трабукко в 1993 г. была предложена оригинальная бесшовная методика герниопластики с использованием жестких пористых протезов специальной формы. Кожный разрез длиной 5-6 см начинается от бугорка лобковой кости и идет параллельно и выше паховой связки. После вскрытия пахового канала семенной канатик мобилизуют и отводят в сторону. При косой паховой грыжи грыжевой мешок после выделения погружают в брюшную полость без вскрытия, прошивания и иссечения. В проекции внутреннего пахового кольца тупо при помощи пальца или катетера Фолея создают ложе в предбрюшинном пространстве, где размещают круглый жесткий полипропиленовый эндопротез, предварительно «надетый» на семенной канатик. При этом хвосты сетки фиксируют между собой полипропиленовым узловым швом. Несколькими рассасывающимися швами поперечную фасцию ушивают над эндопротезом, таким образом, суживая с медиальной стороны внутреннее паховое кольцо. Для того чтобы было можно свободно расположить второй имплантат, выполняют резекцию кремастера. Жесткий полипропиленовый эндопротез размерами 4,5×10 см размещают на задней стенке пахового канала. В результате семенной канатик располагают над сеткой, а на уровне внутреннего пахового кольца - между ее хвостами, широким верхним и нижним узким, которые затем сшивают между собой узловым полипропиленовым швом. Важно, чтобы медиальный край эндопротеза покрывал лобковую кость и ее бугорок на 1,5-2 см. Таким образом, вся задняя стенка пахового канала укреплена сеткой, которую не фиксируют швами к окружающим тканям. Апоневроз наружной косой мышцы ушивают непрерывным нерассасывающимся швом над эндопротезом и под семенным канатиком, который в результате располагается под кожей. Затем накладывают швы на подкожную клетчатку и кожу. В случае прямой паховой грыжи грыжевой мешок также погружают в брюшную полость без вскрытия, прошивания и иссечения. Растянутую поперечную фасцию ушивают непрерывным рассасывающимся погружным швом. В данной ситуации используют только один жесткий полипропиленовый эндопротез, который укладывают на заднюю стенку пахового канала под семенным канатиком по описанной выше методике. (Trabucco Е., Campanelli G. Nuove protesi erniarie in polypropylene // Min. Chir. - 1998. - Vol.53. - P.337-341).In 1993, Trabucco proposed an original seamless technique of hernioplasty using rigid porous prostheses of a special shape. A skin incision 5-6 cm long begins from the tubercle of the pubic bone and runs parallel to and above the inguinal ligament. After opening the inguinal canal, the spermatic cord is mobilized and taken to the side. With oblique inguinal hernia, the hernial sac after discharge is immersed in the abdominal cavity without opening, flashing and excision. In the projection of the internal inguinal ring, a bed is stupidly created with a finger or a Foley catheter in the preperitoneal space, where a round rigid polypropylene endoprosthesis is placed, previously “put on” on the spermatic cord. At the same time, the tails of the mesh are fixed between themselves by a polypropylene nodal seam. With several absorbable sutures, the transverse fascia is sutured over the endoprosthesis, thus narrowing the inner inguinal ring from the medial side. In order to be able to freely position the second implant, a cremaster resection is performed. A rigid polypropylene endoprosthesis with dimensions of 4.5 × 10 cm is placed on the back wall of the inguinal canal. As a result, the spermatic cord is placed above the mesh, and at the level of the internal inguinal ring, between its tails, a wide upper and lower narrow, which are then sutured together by a polypropylene suture. It is important that the medial edge of the endoprosthesis covers the pubic bone and its tubercle by 1.5-2 cm. Thus, the entire posterior wall of the inguinal canal is reinforced with a mesh that is not fixed with sutures to the surrounding tissues. The aponeurosis of the external oblique muscle is sutured with a continuous non-absorbable suture above the endoprosthesis and under the spermatic cord, which is located under the skin as a result. Then suture on the subcutaneous tissue and skin. In the case of a direct inguinal hernia, the hernial sac is also immersed in the abdominal cavity without opening, suturing and excision. The stretched transverse fascia is sutured with a continuous absorbable suture. In this situation, only one rigid polypropylene endoprosthesis is used, which is placed on the posterior wall of the inguinal canal under the spermatic cord according to the method described above. (Trabucco E., Campanelli G. Nuove protesi erniarie in polypropylene // Min. Chir. - 1998. - Vol. 53. - P.337-341).
Достоинством методики является ее бесшовный характер. Результатом является относительно безболевое течение послеоперационного периода. Это позволяет пациентам сразу после операции вставать и постепенно восстанавливать свою двигательную активность. Необходимости в введении наркотических анальгетиков не возникает. Таким образом, данное вмешательство можно выполнять амбулаторно. Уменьшение выраженности болевого синдрома после герниопластики по Трабукко связано с отсутствием натяжения тканей пахового канала. Кроме того, при данном методе не удаляют грыжевой мешок, что сокращает продолжительность и снижает травматичность операции.The advantage of the technique is its seamless nature. The result is a relatively painless postoperative period. This allows patients to immediately get up and gradually restore their motor activity immediately after surgery. The need for the introduction of narcotic analgesics does not arise. Thus, this intervention can be performed on an outpatient basis. A decrease in the severity of pain after hernioplasty according to Trabucco is associated with the absence of tension of the tissues of the inguinal canal. In addition, with this method, the hernial sac is not removed, which reduces the duration and reduces the invasiveness of the operation.
Однако существенным недостатком герниопластики по Трабукко является расположение семенного канатика под кожей, которое нельзя назвать физиологичным. Кроме того, расположение одной из сетчатых пластин в предбрюшинном пространстве усложняет вмешательство.However, a significant drawback of hernioplasty according to Trabucco is the location of the spermatic cord under the skin, which cannot be called physiological. In addition, the location of one of the mesh plates in the preperitoneal space complicates the intervention.
Наиболее близким аналогом к заявляемому изобретению является способ герниопластики по Лихтенштейну с использованием сетчатого протеза, при котором предлагается при фиксации верхнего края сетчатого протеза использовать чрезмышечные швы, включающие поперечную фасцию, внутреннюю косую, поперечную мышцы живота, а также апоневроз наружной косой мышцы живота. (Шурыгин С.Н., Титова Г.П., Чижов Д.В. Исследование механической надежности фиксации имплантата к различным анатомическим структурам паховой области при использовании отдельного или непрерывного шва. // Герниология. - 2004. - №1, с.34-35). При этом в указанной работе на основании экспериментальных исследований сделан вывод, что наибольшей механической прочностью из структур для фиксации сетчатого протеза обладают апоневроз наружной косой мышцы живота и связка Купера.The closest analogue to the claimed invention is a method of hernioplasty according to Liechtenstein using a mesh prosthesis, in which, when fixing the upper edge of the mesh prosthesis, it is proposed to use transmuscular sutures, including transverse fascia, internal oblique, transverse abdominal muscles, as well as aponeurosis of the external oblique muscle of the abdomen. (Shurygin S.N., Titova G.P., Chizhov D.V. Investigation of the mechanical reliability of fixation of the implant to various anatomical structures of the inguinal region using a separate or continuous suture. // Herniology. - 2004. - No. 1, p. 34 -35). Moreover, in this work, on the basis of experimental studies, it was concluded that the aponeurosis of the external oblique muscle of the abdomen and the Cooper ligament have the greatest mechanical strength of the structures for fixing the mesh prosthesis.
Метод, при всех его достоинствах - повышении надежности фиксации верхнего края сетчатого протеза, особенно в условиях повышения внутрибрюшного давления в послеоперационном периоде, обладает и недостатками. Это, прежде всего, сложность наложения швов, проходящих, практически, через всю толщу брюшной стенки. Другим недостатком является все та же возможность захвата в швы вышеуказанных нервов.The method, with all its advantages - increasing the reliability of fixation of the upper edge of the mesh prosthesis, especially in conditions of increasing intra-abdominal pressure in the postoperative period, also has disadvantages. This is, first of all, the difficulty of suturing, passing practically through the entire thickness of the abdominal wall. Another disadvantage is the same possibility of trapping the above nerves in the sutures.
Целью настоящего изобретения является исключение при паховой герниопластике захвата в швы подвздошно-подчревного и подвздошно-пахового нервов и их ветвей и, как следствие, уменьшение болевого синдрома после операции.The aim of the present invention is the exclusion with inguinal hernioplasty capture in the sutures of the ileo-hypogastric and ileo-inguinal nerves and their branches and, as a consequence, the reduction of pain after surgery.
Способ пластики при паховых грыжах, включающий прямой доступ, рассечение апоневроза наружной косой мышцы живота, создание пространства под апоневрозом для размещения сетчатого протеза, выделение паховой связки, семенного канатика, выделение и обработку грыжевого мешка, расположение сетчатого протеза, продольно рассеченного с одного конца, под семенным канатиком, фиксацию его нижнего края швами к паховой связке, медиального края к лонному бугорку и пирамидальной мышце, фиксацию верхнего края, сшивание лоскутов сетчатого протеза между собой и с внутренней косой мышцей живота латеральнее семенного канатика. При этом верхний край сетчатого протеза фиксируют к медиальному лоскуту апоневроза наружной косой мышцы живота с его внутренней стороны по линии, до которой указанный апоневроз отделяют от внутренней косой мышцы живота. Для фиксации верхнего края сетчатого протеза используют сквозные П-образные швы, которые проводят изнутри наружу и завязывают на наружной поверхности апоневроза наружной косой мышцы живота. При этом используют три шва.Plastic surgery for inguinal hernias, including direct access, dissection of the aponeurosis of the external oblique muscle of the abdomen, creation of a space under the aponeurosis to place the mesh prosthesis, allocation of the inguinal ligament, spermatic cord, isolation and processing of the hernial sac, location of the mesh prosthesis, longitudinally dissected from one end, under spermatic cord, fixation of its lower edge with sutures to the inguinal ligament, medial edge to the pubic tubercle and pyramidal muscle, fixation of the upper edge, stitching of the flaps of the mesh prosthesis between wallpaper and with the internal oblique muscle of the abdomen lateral to the spermatic cord. In this case, the upper edge of the mesh prosthesis is fixed to the medial flap of the aponeurosis of the external oblique muscle of the abdomen from its inner side along the line to which the specified aponeurosis is separated from the internal oblique muscle of the abdomen. To fix the upper edge of the mesh prosthesis, through U-shaped sutures are used, which are carried out from the inside out and tied on the outer surface of the aponeurosis of the external oblique muscle of the abdomen. In this case, three seams are used.
Сопоставительный анализ с прототипом позволяет считать, что заявляемый способ соответствует критерию патентоспособности «новизна».Comparative analysis with the prototype suggests that the claimed method meets the criteria of patentability "novelty".
При таком способе оперативного вмешательства швы для фиксации верхнего края сетчатого протеза проводят только через медиальный лоскут апоневроза наружной косой мышцы живота, который с внутренней стороны хорошо визуально контролируется и где захват в швы подвздошно-подчревного, подвздошно-пахового нервов или их ветвей практически исключен. Учитывая высокие прочностные характеристики апоневроза наружной косой мышцы живота выше пахового канала, фиксация верхнего края сетчатого протеза будет во всех случаях достаточной. При этом она будет надежнее, чем при фиксации к сухожильному растяжению внутренней косой мышцы живота (Шурыгин С.Н., Титова Г.П., Чижов Д.В. Исследование механической надежности фиксации имплантата к различным анатомическим структурам паховой области при использовании отдельного или непрерывного шва. // Герниология. - 2004. - №1, с.34-35). В результате снижается выраженность болевых проявлений в послеоперационном периоде. Изменение техники оперативного вмешательства при этом не сказывается на надежности пластики. Внутрибрюшное давление плотно прижимает внутреннюю косую мышцу к сетчатому протезу.With this method of surgical intervention, the sutures for fixing the upper edge of the mesh prosthesis are carried out only through the medial flap of the aponeurosis of the external oblique muscle of the abdomen, which is well visually controlled from the inside and where the capture of the ileo-hypogastric, iliac-inguinal nerves or their branches into the sutures is practically excluded. Given the high strength characteristics of the aponeurosis of the external oblique muscle of the abdomen above the inguinal canal, fixation of the upper edge of the mesh prosthesis will be sufficient in all cases. At the same time, it will be more reliable than when fixing to the tendon extension of the internal oblique muscle of the abdomen (Shurygin S.N., Titova G.P., Chizhov D.V. Investigation of the mechanical reliability of the fixation of the implant to various anatomical structures of the inguinal region using a separate or continuous seam. // Herniology. - 2004. - No. 1, p. 34-35). As a result, the severity of pain manifestations in the postoperative period is reduced. A change in the technique of surgical intervention does not affect the reliability of the plastic. Intra-abdominal pressure tightly presses the internal oblique muscle to the mesh prosthesis.
Все признаки независимого пункта формулы заявляемого способа являются существенными, так как они необходимы для достижения указанного технического результата.All the signs of an independent claim of the claimed method are essential, since they are necessary to achieve the specified technical result.
Признак: - "прямой доступ к паховому каналу " - известен и определяет характер доступа к зоне оперативного воздействия и структуры, через которые он пролегает.Symptom: - "direct access to the inguinal canal" - is known and determines the nature of access to the operative impact zone and the structure through which it passes.
Признак: - " рассечение апоневроза наружной косой мышцы живота, создание пространства под апоневрозом для размещения сетчатого протеза, выделение паховой связки, семенного канатика " - известен, определяет необходимые хирургические действия перед выполнением пластики.Sign: - "dissection of the aponeurosis of the external oblique muscle of the abdomen, the creation of space under the aponeurosis to place the mesh prosthesis, the allocation of the inguinal ligament, spermatic cord" - is known, determines the necessary surgical procedures before performing the plasty.
Признак: - " выделение и обработка грыжевого мешка "- определяет необходимый этап вмешательства на грыжевом мешке.Symptom: - "isolation and processing of the hernial sac" - determines the necessary stage of intervention on the hernial sac.
Признак: - "расположение сетчатого протеза, продольно рассеченного с одного конца, под семенным канатиком, фиксация его нижнего края швами к паховой связке, медиального края к лонному бугорку и пирамидальной мышце, фиксация верхнего края, сшивание лоскутов сетчатого протеза между собой и с внутренней косой мышцей живота латеральнее семенного канатика" - известен, определяет действия, связанные с выполнением собственно пластики.Symptom: - "the location of the mesh prosthesis, longitudinally dissected from one end, under the spermatic cord, fixation of its lower edge with sutures to the inguinal ligament, medial edge to the pubic tubercle and pyramidal muscle, fixation of the upper edge, stitching of the flaps of the mesh prosthesis between themselves and with the internal oblique the abdominal muscle is more lateral than the spermatic cord "- it is known, it determines the actions associated with performing the actual plastic surgery.
Признак: - " верхний край сетчатого протеза фиксируют к медиальному лоскуту апоневроза наружной косой мышцы живота с его внутренней стороны по линии, до которой указанный апоневроз отделяют от внутренней косой мышцы живота" - обеспечивает надежную фиксацию верхнего края сетчатого протеза в зоне визуального контроля без захвата в швы подвздошно-подчревного и подвздошно-пахового нервов. Данный признак из уровня техники не известен.Sign: - "the upper edge of the mesh prosthesis is fixed to the medial flap of the aponeurosis of the external oblique muscle of the abdomen from its inner side along the line to which the specified aponeurosis is separated from the internal oblique muscle of the abdomen" - provides reliable fixation of the upper edge of the mesh prosthesis in the visual control zone without being trapped in sutures of the iliac-hypogastric and iliac-inguinal nerves. This feature is not known from the prior art.
Признак: - " для фиксации верхнего края сетчатого протеза используют сквозные П-образные швы, которые проводят изнутри наружу и завязывают на наружной поверхности апоневроза наружной косой мышцы живота"- обеспечивает более простое и быстрое наложение швов для фиксации верхнего края сетчатого протеза при паховой герниопластике.Sign: - "for fixing the upper edge of the mesh prosthesis, through U-shaped sutures are used, which are carried out from the inside out and tied to the external surface of the aponeurosis of the external oblique muscle of the abdomen" - provides a simpler and faster suturing for fixing the upper edge of the mesh prosthesis with inguinal hernioplasty.
Данный признак из уровня техники не известен.This feature is not known from the prior art.
Признак:- "для фиксации верхнего края сетчатого протеза используют три шва "- является новым и определяет минимальное и достаточное количество шовного материала для фиксации верхнего края сетчатого протеза.Symptom: - “three sutures are used to fix the upper edge of the mesh prosthesis” - is new and determines the minimum and sufficient amount of suture material to fix the upper edge of the mesh prosthesis.
При взаимодействии существенных признаков получается новый технический результат, а именно достижение надежной герниопластики без прошивания внутренней косой мышцы живота в зоне расположения подвздошно-подчревного и подвздошно-пахового нервов.In the interaction of essential features, a new technical result is obtained, namely, the achievement of reliable hernioplasty without flashing the internal oblique muscle of the abdomen in the area of the ileo-hypogastric and ileo-inguinal nerves.
Три из семи отличительных признаков заявляемого способа из уровня техники не известны. Следовательно, заявляемое техническое решение соответствует критерию «изобретательский уровень».Three of the seven distinctive features of the proposed method from the prior art are not known. Therefore, the claimed technical solution meets the criterion of "inventive step".
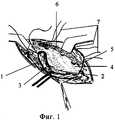
На фиг.1 показан способ фиксации швами сетчатого протеза к медиальному лоскуту апоневроза наружной косой мышцы живота. На фиг.2 фиксирующие швы завязаны.Figure 1 shows a method of fixing sutures of a mesh prosthesis to a medial flap of aponeurosis of the external oblique muscle of the abdomen. In figure 2, the locking seams are tied.
Предлагаемый способ операции при паховой грыже осуществляется следующим образом. Выполняют разрез кожи и подкожной клетчатки длиной 4-6 см в проекции пахового канала над паховой складкой. Рассекают апоневроз наружной косой мышцы живота 1. По вскрытии апоневроза препаровочным тупфером выделяют паховую связку 2, семенной канатик 3, край внутренней косой мышцы на 2-3 см и лонный бугорок (на чертеже не обозначены). Тупо пальцем выделяют пространство под апоневрозом вверх по ходу разреза для последующего размещения сетчатого протеза. Выделяют и обрабатывают грыжевой мешок (на чертеже не обозначен). Сетчатый протез 4 моделируют, продольно рассекают с одного конца и укладывают под семенной канатик 3 так, чтобы в его разрезе свободно поместился семенной канатик 3. Сетчатый протез 4 фиксируют непрерывным проленовым швом к паховой связке 2. Затем верхний край сетки фиксируют отдельными П-образными сквозными швами 7 к медиальному лоскуту 5 апоневроза наружной косой мышцы живота с его внутренней стороны по линии, до которой указанный апоневроз отделяют от внутренней косой мышцы живота 6. После этого лоскуты сетчатого протеза 4 сшивают друг с другом и с внутренней косой мышцей латеральнее семенного канатика 3. На фиг.2 швы для фиксации верхнего края сетчатого протеза завязаны. Затем приступают к формированию передней стенки пахового канала и послойному ушиванию кожи и подкожной клетчатки.The proposed method of operation for inguinal hernia is as follows. An incision is made of the skin and subcutaneous tissue 4-6 cm long in the projection of the inguinal canal above the inguinal fold. Dissection of the aponeurosis of the external oblique muscle of the abdomen 1. After opening the aponeurosis with the preparation tuffer, the
В 1-м хирургическом отделении Дорожной клинической больницы на ст. Иркутск - пассажирский выполнено 21 грыжесечение у мужчин при косых и прямых паховых грыжах с использованием предложенного способа. В 9 случаях грыжи носили прямой характер, у 12 пациентов были косыми. В качестве синтетического протеза использовались сетки фирмы Линтекс. Срок наблюдения - до 9 мес. Во всех случаях после выполнения пластики в предложенном варианте после операции болевой синдром был минимально выражен. Послеоперационный период во всех случаях прошел без осложнений. Рецидивов не отмечено.In the 1st surgical department of the Road Clinical Hospital at st. Irkutsk - passenger performed 21 hernia repair in men with oblique and direct inguinal hernias using the proposed method. In 9 cases, hernias were direct, in 12 patients they were oblique. Lintex nets were used as a synthetic prosthesis. The observation period is up to 9 months. In all cases, after performing plastic surgery in the proposed embodiment, after surgery, the pain syndrome was minimally expressed. The postoperative period in all cases passed without complications. No relapses were noted.
Claims (3)
Translated fromRussianPriority Applications (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| RU2008114794/14ARU2371106C1 (en) | 2008-04-15 | 2008-04-15 | Inguinal hernia repair technique |
Applications Claiming Priority (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| RU2008114794/14ARU2371106C1 (en) | 2008-04-15 | 2008-04-15 | Inguinal hernia repair technique |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| RU2371106C1true RU2371106C1 (en) | 2009-10-27 |
Family
ID=41352956
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| RU2008114794/14ARU2371106C1 (en) | 2008-04-15 | 2008-04-15 | Inguinal hernia repair technique |
Country Status (1)
| Country | Link |
|---|---|
| RU (1) | RU2371106C1 (en) |
Cited By (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2502479C1 (en)* | 2012-08-10 | 2013-12-27 | Сергей Владимирович Шалашов | Method of large ventral postoperative hernia plasty |
Citations (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2299691C1 (en)* | 2006-01-10 | 2007-05-27 | ГОУ ВПО Омская Государственная Медицинская Академия | Interfacial plasty method for treating inguinal hernia cases aggravated with connective tissue dysplasia |
| RU2303403C1 (en)* | 2005-10-31 | 2007-07-27 | Евгений Сергеевич Петров | Method for carrying out inguinal canal combined plastic repair without tension |
- 2008
- 2008-04-15RURU2008114794/14Apatent/RU2371106C1/ennot_activeIP Right Cessation
Patent Citations (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2303403C1 (en)* | 2005-10-31 | 2007-07-27 | Евгений Сергеевич Петров | Method for carrying out inguinal canal combined plastic repair without tension |
| RU2299691C1 (en)* | 2006-01-10 | 2007-05-27 | ГОУ ВПО Омская Государственная Медицинская Академия | Interfacial plasty method for treating inguinal hernia cases aggravated with connective tissue dysplasia |
Non-Patent Citations (2)
| Title |
|---|
| Ненатяжная герниопластика./ Под ред. В.Н.ЕГИЕВА. - М.: Медпрактика, 2002, с.73-86. PAPAZIOGAS В. Tension-free repair versus modified Bassini technique (Andrewe technique) for strangulated ingunal hernia: a comparative study. - Hernia. 2005, May; 9(2): 156-9. Epub 2005 Feb 3 (Abstract). LANGENBACH M.R. Comparison of biomateriais: three meshes and TAPP for inguinal hernia. Surg Endose. 2006 Oct; 20(10):155-7. Epub 2006 aug 16 (Abstract).* |
| ШУРЫГИН С.Н. и др. Исследование механической надежности фиксации имплантата к различным анатомическим структурам паховой области при использовании отдельного или напрерывного шва. Герниология, 2004, 1, 34-35.* |
Cited By (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2502479C1 (en)* | 2012-08-10 | 2013-12-27 | Сергей Владимирович Шалашов | Method of large ventral postoperative hernia plasty |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| RU2432912C1 (en) | Method of endoscopic plasty in case of inguinal hernias | |
| RU2324427C2 (en) | Method of combined plastic surgery of large and giant median ventral hernia | |
| RU2384301C1 (en) | Inguinal canal plasty technique | |
| RU2452405C1 (en) | Method of plasty in case of inguinal hernias | |
| RU2398526C1 (en) | Method of combined hernioventroplasty of median ventral hernias | |
| RU2371106C1 (en) | Inguinal hernia repair technique | |
| RU2066125C1 (en) | Method for carrying out plastic restoration of gross defects of anterior abdominal wall | |
| RU2289323C2 (en) | Method for tension-free hernioplasty in case of inguinal hernias | |
| RU2349265C2 (en) | Method of surgical treatment of indirect inguinal hernia | |
| RU2502483C1 (en) | Method of plasty in case of inguinal hernias | |
| RU2685682C1 (en) | Method for surgical management of postoperative and recurrent ventral hernias | |
| RU2147421C1 (en) | Method for rebuilding abdominal wall in cases of inguinal and femoral hernia | |
| RU2403876C1 (en) | Method of surgical management of medium indirect and direct inguinal hernias | |
| RU2261051C2 (en) | Surgical method for treating the cases of postoperative median ventral hernias | |
| RU2581249C1 (en) | Method for repair of anterior abdominal wall desmoid fibroma rectus | |
| RU2585734C1 (en) | Method for operation of inguinal hernias | |
| RU2422105C1 (en) | Method of hernioplasty in case of large and gigantic post-operational hernias by alcharyshkin | |
| RU2286721C1 (en) | Method for surgical treatment of inguinal hernias | |
| RU2324432C1 (en) | Method of plastic surgery of posterior wall of inguinal canal with two-ply endoprosthesis with use of endoscopic equipment | |
| RU2825698C1 (en) | Method for repair of mid-lateral postoperative ventral hernias | |
| RU2284761C1 (en) | Method for surgical treatment of inguinal hernia | |
| RU2254063C2 (en) | Method for surgical treatment of postoperative ventral hernias | |
| RU2715095C1 (en) | Method of surgical treatment of patients with large and giant ventral hernias | |
| RU2254062C2 (en) | Method for surgical therapy of median postoperative ventral hernias in hypogastric area | |
| RU2321356C1 (en) | Method of plasty at inguinal hernias |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| MM4A | The patent is invalid due to non-payment of fees | Effective date:20110416 |