RU2336043C1 - Method of surgical treatment of achilles tendon rupture - Google Patents
Method of surgical treatment of achilles tendon ruptureDownload PDFInfo
- Publication number
- RU2336043C1 RU2336043C1RU2007115971/14ARU2007115971ARU2336043C1RU 2336043 C1RU2336043 C1RU 2336043C1RU 2007115971/14 ARU2007115971/14 ARU 2007115971/14ARU 2007115971 ARU2007115971 ARU 2007115971ARU 2336043 C1RU2336043 C1RU 2336043C1
- Authority
- RU
- Russia
- Prior art keywords
- tendon
- achilles tendon
- insert
- achilles
- surgical treatment
- Prior art date
Links
Images


Landscapes
- Acyclic And Carbocyclic Compounds In Medicinal Compositions (AREA)
Abstract
Description
Translated fromRussianИзобретение относится к медицине, а именно к травматологии в лечении разрыва ахиллова сухожилия.The invention relates to medicine, namely to traumatology in the treatment of Achilles tendon rupture.
Известны разные способы хирургического лечения разрывов ахиллова сухожилия.There are various methods of surgical treatment of Achilles tendon ruptures.
Например, способ Чернавского (И.А.Мовшович. Оперативная ортопедия. М., 1994, стр.319) заключается в выкраивании П-образного лоскута из сухожильного растяжения икроножной мышцы с ножкой на дистальном конце. Этот лоскут выводят на заднюю поверхность сухожилия и перекрывают им дефект. Недостатки способа: не восстанавливается сухожильно-мышечное натяжение, не используется рубцовая ткань для укрепления трансплантата.For example, the Chernavsky method (I. A. Movshovich. Operational orthopedics. M., 1994, p. 319) consists in cutting a U-shaped flap from a tendon extension of the calf muscle with a leg at the distal end. This flap is brought to the posterior surface of the tendon and overlap with it the defect. The disadvantages of the method: the tendon-muscle tension is not restored, scar tissue is not used to strengthen the graft.
Способ С.И.Двойникова (а.с. №1191065 от 15.11.85 г.) предусматривает иссечение рубца сшивания концов сухожилия капроном или лавсаном, укрепление швов сухожилием подошвенной мышцы. Недостатки способа: сухожилие подошвенной мышцы интимно спаяно с сухожилием трехглавой мышцы (А.В.Краев. Анатомия человека. М., 1978, №1, стр.281), поэтому обычно разрывается одновременно с ахилловым сухожилием; швами и тонким сухожилием подошвенной мышцы трудно удержать ретрагированную трехглавую мышцу голени в заданном положении.The method of S.I.Dvoinikov (A.S. No. 1191065 dated 11/15/85) provides for excision of the scar of suturing of the ends of the tendon with a capron or lavsan, strengthening of sutures with a tendon of the plantar muscle. The disadvantages of the method: the tendon of the plantar muscle is intimately soldered to the tendon of the triceps muscle (A.V. Kraev. Human Anatomy. M., 1978, No. 1, p. 281), therefore, it usually breaks at the same time as the Achilles tendon; with sutures and a thin tendon of the plantar muscle, it is difficult to keep the retracted triceps muscle of the lower leg in a given position.
По способу А.Ф.Краснова (а.с. №668674 от 25.06.79 г.) используют П-образный лоскут и часть рубца для пластики. Рубец выделяют и в нем формируют углубления в виде "футляра". Лоскут проводят на переднюю поверхность сухожилия, помещают в "футляр" рубцовой ткани и фиксируют в расщеп дистального конца сухожилия. Недостаток такого способа заключается в том, что не восстанавливается оптимальное сухожильно-мышечное натяжение (тонус трехглавой мышцы голени). Восстановление оптимального натяжения сухожильно-мышечного комплекса имеет решающее значение в сухожильно-мышечной пластике (И.А.Мовшович. Оперативная ортопедия. М., 1994, стр.22; А.Ф.Краснов, Г.П.Котельников, А.П.Чернов. Сухожильно-мышечная пластика в травматологии и ортопедии. Самара, 1999, стр.215).According to the method of A.F. Krasnov (AS No. 668674 dated 06/25/79), a U-shaped flap and part of the scar for plastic are used. The scar is isolated and recesses are formed in it in the form of a “case”. The flap is carried out on the front surface of the tendon, placed in a “case” of scar tissue and fixed in the cleft of the distal end of the tendon. The disadvantage of this method is that the optimal tendon-muscle tension (tonus of the triceps muscle of the leg) is not restored. The restoration of the optimal tension of the tendon-muscle complex is crucial in tendon-muscle plastic surgery (I.A. Movshovich. Operative orthopedics. M., 1994, p. 22; A.F. Krasnov, G.P. Kotelnikov, A.P. Chernov, Tendon-muscle plastic surgery in traumatology and orthopedics, Samara, 1999, p. 215).
При значительном растяжении, разволокнении тканей сухожилия выполняют пластическое восстановление разгибательного аппарата с использованием алло- и аутотканей. Полосу капроновой или лавсановой ткани, соответствующей зоне повреждения, фиксируют к передней поверхности разгибателя голени, покрывая зону сухожильного растяжения (А.Ф.Краснов, В.М.Аршин, М.Д.Цейтлин. Справочник по травматологии. М.: Медицина, 1984, стр.308). Недостаток данного способа, при котором используются биосовместимые искусственные материалы (лавсановые, капроновые, углесодержащие ленты) для пластического восстановления ахиллова сухожилия, заключается в сравнительно долгом процессе заживления: от 1,5 до 3 месяцев.With significant stretching, razvolennosti tendon tissues perform plastic restoration of the extensor apparatus using allo and autotissues. The strip of kapron or lavsan tissue corresponding to the damage zone is fixed to the front surface of the extensor tibia, covering the tendon extension zone (A.F. Krasnov, V.M. Arshin, M.D. Zeitlin. Handbook of Traumatology. M .: Medicine, 1984 p. 308). The disadvantage of this method, which uses biocompatible artificial materials (lavsan, kapron, carbon-containing tapes) for plastic restoration of the Achilles tendon, is a relatively long healing process: from 1.5 to 3 months.
Наиболее близким к предлагаемому является способ хирургического лечения застарелых разрывов ахиллова сухожилия по патенту RU №2230507, МПК А61В 17/56, 2004.06.20, позволяющий восстановить разорванное сухожилие с использованием рубца и сухожильного лоскута, сложенного вдвое, улучшить функцию трехглавой мышцы голени путем создания оптимального сухожильно-мышечного натяжения. Сущность способа: из сухожильного растяжения икроножной мышцы, рубцового регенерата и ахиллова сухожилия выкраивают лоскут на ножке длиной 18-20 см. Лоскут отводят книзу, на проксимальный и дистальный концы ахиллова сухожилия и рубцовый регенерат накладывают переплетающийся шов Кюнео.Closest to the proposed is a method of surgical treatment of chronic Achilles tendon ruptures according to patent RU No. 2230507, IPC АВВ 17/56, 2004.06.20, which allows to restore a torn tendon using a scar and a tendon flap folded in half, to improve the function of the triceps muscle of the lower leg by creating the optimal tendon-muscle tension. The essence of the method: from a tendon stretch of the calf muscle, cicatricial regenerate and Achilles tendon, a flap on a leg 18-20 cm long is cut out. The flap is brought down, the proximal and distal ends of the Achilles tendon and cicatricial regenerate impose an interlocking suture of Kuneo.
Недостаток способа: травмируется собственное ахиллово сухожилие.The disadvantage of this method is injured own Achilles tendon.
Для исправления выявленного недостатка была поставлена задача: повысить эффективность лечения разрыва ахиллова сухожилия за счет уменьшения травматичности способа и сокращения сроков лечения.To correct the identified deficiency, the task was set: to increase the effectiveness of treatment of Achilles tendon rupture by reducing the invasiveness of the method and shortening the treatment time.
Поставленная задача достигается следующим образом.The task is achieved as follows.
При оперативном лечении разрыва ахиллова сухожилия, включающем использование сложенной вдвое вставки из гомотрансплантата с фиксацией ее к дистальному (нижнему) концу ахиллова сухожилия, согласно изобретению, вставку формируют из консервированной твердой мозговой оболочки, загибают торцы вставки с обеих сторон и прошивают, в концах разорванного сухожилия делают продольные разрезы, через которые вводится вставка, с последующей фиксацией ее к проксимальному (верхнему) концу ахиллова сухожилия и наложением наводящих швов на концы разорванного сухожилия.In the surgical treatment of Achilles tendon rupture, including the use of a double folded insert from a homotransplant with its fixation to the distal (lower) end of the Achilles tendon, according to the invention, the insert is formed from a preserved dura mater, the ends of the insert are bent on both sides and stitched, at the ends of the torn tendon make longitudinal sections through which the insert is inserted, with its subsequent fixation to the proximal (upper) end of the Achilles tendon and overlaying sutures at the ends of the gap annogo tendon.
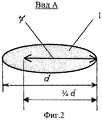
Сущность способа поясняется чертежами, где изображено: на фиг.1 - поврежденное сухожилие; на фиг.2 - поперечное сечение сухожилия с разрезом (вид А на фиг.1). На фиг.3-4 показано формирование вставки из консервированной твердой мозговой оболочки: на фиг.3 - складывание вставки вдвое; на фиг.4 - складывание вставки по торцам.The essence of the method is illustrated by drawings, which depict: in Fig.1 - damaged tendon; figure 2 is a cross section of a tendon with a section (view a in figure 1). Figure 3-4 shows the formation of the insert from canned dura mater: figure 3 - folding the insert in half; figure 4 - folding inserts at the ends.
На чертежах обозначено: 1 - верхний (проксимальный) конец ахиллова сухожилия; 2 - нижний (дистальный) конец ахиллова сухожилия; 3 - вставка из ТМО; 4 - швы фиксации верхнего конца ахиллова сухожилия; 5 - швы фиксации нижнего конца ахиллова сухожилия; 6 - продольный разрез в сухожилиях; 7 - глубина разрезов в сухожилиях; d - диаметр сухожилия.The drawings indicate: 1 - the upper (proximal) end of the Achilles tendon; 2 - the lower (distal) end of the Achilles tendon; 3 - insert from TMT; 4 - sutures for fixation of the upper end of the Achilles tendon; 5 - sutures for fixation of the lower end of the Achilles tendon; 6 - a longitudinal section in the tendons; 7 - the depth of cuts in the tendons; d is the diameter of the tendon.
Способ выполняют следующим образом.The method is as follows.
Для доступа к ахиллову сухожилию линейным, параллельным сухожилию разрезом по задней поверхности голени рассекают кожу и подкожную клетчатку вместе с паратеноном длиной 10-12 см и выделяют на всем протяжении разреза ахиллово сухожилие. После освежевания концов разорванного сухожилия в их концах делается глубокий продольный разрез длиной 20-30 мм каждый (фиг.1), а глубина разреза составляет примерно3/4 от диаметра d самого сухожилия (фиг.2). Из гомотрансплантата консервированной твердой мозговой оболочки (ТМО) делается вставка прямоугольной формы, соответствующей зоне повреждения. Забор и консервация ТМО проводится, например, в лаборатории забора и консервации тканей НИИТО г.Нижнего Новгорода. Вставка складывается вдвое по длине (фиг.3) в ленту, шириной 10-15 мм (в зависимости от ширины ахиллова сухожилия) и прошивается редкими узловыми швами. Торцевые концы вставки загибаются на длину не менее 5 мм (фиг.4) и прошиваются с каждой стороны по концам лавсановыми лигатурами с длиной оставленных концов 100-150 мм. Затем вставка вводится верхним концом в разрез проксимального (верхнего) конца сухожилия (на длину разреза) и фиксируется двумя глубокими погружными швами (фиг.1), при этом с помощью иглы на переднюю поверхность разреза через вершину выводят лигатуры (нити) вставки с каждого ее конца. Стопу выводят в положение максимального сгибания. После чего зафиксированная в верхнем конце сухожилия вставка втягивается в разрез в дистальном (нижнем) конце поврежденного сухожилия. Концы лигатур натягивают до такого состояния, чтобы дистальный и проксимальный концы ахиллова сухожилия максимально приблизились друг к другу. При этом восстанавливается сухожильно-мышечное натяжение, утраченное вследствие расхождения концов ахиллова сухожилия. Вставка из ТМО фиксируется в нижнем конце сухожилия двумя глубокими погружными швами (аналогично верхнему концу сухожилия), перекрывая область разреза. Целостность сухожилия восстанавливается путем зашивания (после тщательного гемостаза) продольных разрезов сухожилий с наложением наводящих швов на концы сухожилий. После операции накладывают подкладочную гипсовую повязку от кончиков пальцев до верхней трети бедра, при этом стопу сгибают до угла 130°, а голень до угла 150°. Срок иммобилизации 5 недель.To access the Achilles tendon, a linear parallel to the tendon incision along the posterior surface of the lower leg cuts the skin and subcutaneous tissue together with paratenon 10-12 cm long and secures the Achilles tendon throughout the incision. After osvezhevaniya torn tendon ends at their ends is a longitudinal sectional view of a deep 20-30 mm length (1), and the cut depth is about3/4 of the diameter d of the tendon (Figure 2). A rectangular insert corresponding to the damage zone is made from a homotransplant of canned dura mater (TMO). The collection and preservation of TMT is carried out, for example, in the laboratory for the collection and preservation of tissues of NIITO in Nizhny Novgorod. The insert is folded twice in length (Fig. 3) into a tape, 10-15 mm wide (depending on the width of the Achilles tendon) and stitched with rare interrupted sutures. The end ends of the insert are bent to a length of at least 5 mm (Fig. 4) and are stitched on each side at the ends with lavsan ligatures with the length of the left ends 100-150 mm. Then the insertion is introduced by the upper end into the incision of the proximal (upper) end of the tendon (to the length of the incision) and is fixed with two deep immersion sutures (Fig. 1), while using the needle on the front surface of the incision, the ligatures (filaments) of the insert are removed from each the end. The foot is brought to the maximum flexion position. After that, the insert fixed in the upper end of the tendon is drawn into the incision in the distal (lower) end of the damaged tendon. The ends of the ligatures are pulled to such a state that the distal and proximal ends of the Achilles tendon are as close as possible to each other. This restores the tendon-muscle tension lost due to the divergence of the ends of the Achilles tendon. An insert of TMT is fixed at the lower end of the tendon with two deep immersion sutures (similar to the upper end of the tendon), overlapping the incision area. The integrity of the tendon is restored by suturing (after careful hemostasis) longitudinal sections of the tendons with suturing the ends of the tendons. After the operation, a lining gypsum dressing is applied from the tips of the fingers to the upper third of the thigh, while the foot is bent to an angle of 130 °, and the lower leg to an angle of 150 °. The immobilization period is 5 weeks.
Принципиальное отличие предложенного способа от известного заключается в формировании вставки из консервированной твердой мозговой оболочки, фиксации ее к ее к дистальному и проксимальному концу ахиллова сухожилия в положении с загнутыми торцами вставки для увеличения прочности и укрепления места разрыва сухожилия. Причем завернутая часть вставки, находясь между однородными тканями, быстрее перестраивает свою структуру в послеоперационном периоде. Данный способ позволяет осуществить быстрое вживление и рассасывание мозговой оболочки вставки, что позволяет значительно сократить сроки срастания сухожилия, исключив его дополнительное травмирование.The fundamental difference between the proposed method and the known one consists in forming an insert from a canned dura mater, fixing it to it at the distal and proximal end of the Achilles tendon in the position with the insert ends curved to increase strength and strengthen the tendon rupture site. Moreover, the wrapped part of the insert, being between homogeneous tissues, quickly rebuilds its structure in the postoperative period. This method allows for quick implantation and resorption of the medulla of the insert, which can significantly reduce the time of fusion of the tendon, eliminating its additional injury.
Предложенным способом с положительным эффектом было оперировано 12 больных. Признаков стеноза в послеоперационный период не обнаружено.The proposed method with a positive effect was operated on 12 patients. There were no signs of stenosis in the postoperative period.
Клинический пример 1. Больной Т., 33 года, поступил в больницу с диагнозом: повторный подкожный разрыв правого ахиллова сухожилия с формированием посттравматической внутристволовой кисты. Произведена операция по предложенному способу (выполнена пластика ахиллова сухожилия твердой мозговой оболочки). Через две недели сняты швы, заживление первичным натяжением, наложена циркулярная гипсовая повязка. Через месяц снята иммобилизация, приступил к работе.Clinical example 1. Patient T., 33 years old, was admitted to the hospital with a diagnosis of repeated subcutaneous rupture of the right Achilles tendon with the formation of a post-traumatic intrastemal cyst. The operation was performed according to the proposed method (performed plastic Achilles tendon of the dura mater). Two weeks later, the sutures were removed, healing by primary intention, a circular plaster cast was applied. A month later, the immobilization was lifted, I started to work.
Клинический пример 2. Больной Д., 32 года, поступил в больницу с диагнозом: полный подкожный разрыв правого ахиллова сухожилия. Проведена операция по предложенному способу. Результат положительный. Через девять дней сняты швы, заживление первичным натяжением, наложена циркулярная гипсовая повязка. Через месяц снята иммобилизация, приступил к работе.Clinical example 2. Patient D., 32 years old, was admitted to the hospital with a diagnosis of complete subcutaneous rupture of the right Achilles tendon. The operation according to the proposed method. The result is positive. Nine days later, the sutures were removed, healing by first intention, a circular plaster cast was applied. A month later, the immobilization was lifted, I started to work.
Способ может быть рекомендован в практическую медицину.The method can be recommended in practical medicine.
Claims (1)
Translated fromRussianPriority Applications (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| RU2007115971/14ARU2336043C1 (en) | 2007-04-26 | 2007-04-26 | Method of surgical treatment of achilles tendon rupture |
Applications Claiming Priority (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| RU2007115971/14ARU2336043C1 (en) | 2007-04-26 | 2007-04-26 | Method of surgical treatment of achilles tendon rupture |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| RU2336043C1true RU2336043C1 (en) | 2008-10-20 |
Family
ID=40041130
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| RU2007115971/14ARU2336043C1 (en) | 2007-04-26 | 2007-04-26 | Method of surgical treatment of achilles tendon rupture |
Country Status (1)
| Country | Link |
|---|---|
| RU (1) | RU2336043C1 (en) |
Cited By (3)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2502481C1 (en)* | 2012-10-24 | 2013-12-27 | Федеральное государственное бюджетное учреждение "Центральный научно-исследовательский институт травматологии и ортопедии имени Н.Н. Приорова" Министерства здравоохранения Российской Федерации (ФГБУ "ЦИТО им. Н.Н. Приорова" Минздрава России) | Method of surgical treatment of old achilles tendon ruptures |
| RU2537888C1 (en)* | 2013-10-11 | 2015-01-10 | Государственное бюджетное образовательное учреждение высшего профессионального образования "Самарский государственный медицинский университет" Министерства здравоохранения Российской Федерации | Method for surgical management of old achilles tendon rupture |
| RU2627293C1 (en)* | 2016-10-26 | 2017-08-04 | федеральное государственное автономное образовательное учреждение высшего образования "Российский университет дружбы народов" (РУДН) | Method for achilles tendon plasty |
Citations (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2230507C2 (en)* | 2002-01-25 | 2004-06-20 | Самарский государственный медицинский университет | Method for surgical treatment of old ruptures of achilles tendon |
| RU2289345C1 (en)* | 2005-09-06 | 2006-12-20 | Федеральное государственное учреждение "Нижегородский научно-исследовательский институт травматологии и ортопедии Федерального агентства по здравоохранению и социальному развитию" | Surgical method for treating the cases of inveterate ruptures of achilles tendon |
- 2007
- 2007-04-26RURU2007115971/14Apatent/RU2336043C1/ennot_activeIP Right Cessation
Patent Citations (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2230507C2 (en)* | 2002-01-25 | 2004-06-20 | Самарский государственный медицинский университет | Method for surgical treatment of old ruptures of achilles tendon |
| RU2289345C1 (en)* | 2005-09-06 | 2006-12-20 | Федеральное государственное учреждение "Нижегородский научно-исследовательский институт травматологии и ортопедии Федерального агентства по здравоохранению и социальному развитию" | Surgical method for treating the cases of inveterate ruptures of achilles tendon |
Non-Patent Citations (1)
| Title |
|---|
| МОВШОВИЧ И.А. Оперативная ортопедия. - М.: Медицина, 1994, 2-е изд., с.319, 320. GARNETIN "Bilateral Achilles tendon rupture: a case report" Accid Emerg Nurs. 2005 Oct; 13(4): 220-3. Epub 2005 Oct 4 (Abstract).* |
Cited By (3)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2502481C1 (en)* | 2012-10-24 | 2013-12-27 | Федеральное государственное бюджетное учреждение "Центральный научно-исследовательский институт травматологии и ортопедии имени Н.Н. Приорова" Министерства здравоохранения Российской Федерации (ФГБУ "ЦИТО им. Н.Н. Приорова" Минздрава России) | Method of surgical treatment of old achilles tendon ruptures |
| RU2537888C1 (en)* | 2013-10-11 | 2015-01-10 | Государственное бюджетное образовательное учреждение высшего профессионального образования "Самарский государственный медицинский университет" Министерства здравоохранения Российской Федерации | Method for surgical management of old achilles tendon rupture |
| RU2627293C1 (en)* | 2016-10-26 | 2017-08-04 | федеральное государственное автономное образовательное учреждение высшего образования "Российский университет дружбы народов" (РУДН) | Method for achilles tendon plasty |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| RU2195892C2 (en) | Method for surgical treatment of cross-sectional foot spreading and varus defect of the great toe | |
| RU2336043C1 (en) | Method of surgical treatment of achilles tendon rupture | |
| RU2343862C2 (en) | Method of autoplasty of own ligament of whirlbone after endoprosthesis replacement of knee joint | |
| RU2230507C2 (en) | Method for surgical treatment of old ruptures of achilles tendon | |
| RU2138214C1 (en) | Method for applying tendinoplastic repair of finger flexors | |
| RU2317035C2 (en) | Method for autoplasty of the lesions of lateral group of talocrural joint ligaments | |
| RU2210334C1 (en) | Method for combined plasty of thumb's stump | |
| RU2124327C1 (en) | Method of treating closed fractures of patellae ligament | |
| RU2201160C2 (en) | Method for restoration of achilles tendon at ruptures | |
| RU2391053C1 (en) | Method of surgical treatment of posttraumatic strictures of urethra | |
| Park et al. | Strategic considerations on the configuration of free flaps and their vascular pedicles combined with Ilizarov distraction in the lower extremity | |
| RU2195875C2 (en) | Method for the plasty of peripheral nerves' defects at combined deformations of limbs | |
| RU2340303C2 (en) | Method of prosthetics of tendons | |
| RU2668466C1 (en) | Method for treatment of degenerative and chronic achilles tendon | |
| RU2340301C2 (en) | Method of achilles tendon plasty | |
| RU2578377C2 (en) | Method for surgical restoration of chronic achilles tendon rupture | |
| RU2157663C2 (en) | Method for fixing phalloprosthesis | |
| RU2417773C1 (en) | Method for reconstructing tendon of quadriceps muscle of thigh | |
| RU2791972C1 (en) | Method for treatment of osteomyelitis of calcaneus based on lipofibrous autograft | |
| RU2826853C1 (en) | Method for reconstructing tongue and floor of oral cavity after glossectomy | |
| RU2779219C1 (en) | Method for treating massive tears of tendons of the shoulder rotator cuff | |
| RU2776216C1 (en) | Method for performing autoplasty of long-standing injury of the achilles tendon | |
| RU2828558C1 (en) | Method of nasal dorsum bones reinforcement by their fixation with suspended suture | |
| RU2760844C1 (en) | Method for cross-tendon stitching of the anterior sections of the supraspinatus tendon with incomplete (partial) ruptures from the articular surface | |
| RU2385151C1 (en) | Tibial cavities plasty technique in surgical treatment of chronic osteomyelitis |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| MM4A | The patent is invalid due to non-payment of fees | Effective date:20090427 |