RU2334481C1 - Method for treatment of temporomandibular joint ankylose and lower micrognathia in children - Google Patents
Method for treatment of temporomandibular joint ankylose and lower micrognathia in childrenDownload PDFInfo
- Publication number
- RU2334481C1 RU2334481C1RU2006144517/14ARU2006144517ARU2334481C1RU 2334481 C1RU2334481 C1RU 2334481C1RU 2006144517/14 ARU2006144517/14 ARU 2006144517/14ARU 2006144517 ARU2006144517 ARU 2006144517ARU 2334481 C1RU2334481 C1RU 2334481C1
- Authority
- RU
- Russia
- Prior art keywords
- distraction
- branch
- jaw
- children
- compression
- Prior art date
Links
- 238000000034methodMethods0.000titleclaimsabstractdescription24
- 206010023198Joint ankylosisDiseases0.000titleclaimsdescription14
- 210000001738temporomandibular jointAnatomy0.000titleclaimsdescription13
- 206010027543MicrognathiaDiseases0.000titleclaimsdescription11
- 208000002598MicrognathismDiseases0.000titleclaimsdescription11
- 230000008569processEffects0.000claimsabstractdescription10
- 239000012634fragmentSubstances0.000claimsabstractdescription9
- 238000002271resectionMethods0.000claimsabstractdescription4
- 208000008822AnkylosisDiseases0.000claimsdescription13
- 210000002176pterygoid muscleAnatomy0.000claimsdescription8
- 230000008468bone growthEffects0.000claimsdescription5
- 210000000988bone and boneAnatomy0.000abstractdescription17
- 239000003814drugSubstances0.000abstractdescription3
- 230000036770blood supplyEffects0.000abstractdescription2
- 210000003205muscleAnatomy0.000abstractdescription2
- 210000004373mandibleAnatomy0.000abstract3
- 230000006835compressionEffects0.000abstract1
- 238000007906compressionMethods0.000abstract1
- 239000000126substanceSubstances0.000abstract1
- 206010052428WoundDiseases0.000description5
- 208000027418Wounds and injuryDiseases0.000description5
- 238000001356surgical procedureMethods0.000description4
- 230000000735allogeneic effectEffects0.000description3
- 230000002500effect on skinEffects0.000description3
- 230000014759maintenance of locationEffects0.000description3
- 210000000966temporal muscleAnatomy0.000description3
- ZOXJGFHDIHLPTG-UHFFFAOYSA-NBoronChemical compound[B]ZOXJGFHDIHLPTG-UHFFFAOYSA-N0.000description2
- 229910052796boronInorganic materials0.000description2
- 239000002729catgutSubstances0.000description2
- 230000007547defectEffects0.000description2
- 230000011164ossificationEffects0.000description2
- 230000002980postoperative effectEffects0.000description2
- 206010002091AnaesthesiaDiseases0.000description1
- 208000032170Congenital AbnormalitiesDiseases0.000description1
- 206010010356Congenital anomalyDiseases0.000description1
- VGGSQFUCUMXWEO-UHFFFAOYSA-NEtheneChemical compoundC=CVGGSQFUCUMXWEO-UHFFFAOYSA-N0.000description1
- 239000005977EthyleneSubstances0.000description1
- 230000009471actionEffects0.000description1
- 230000004913activationEffects0.000description1
- 230000037005anaesthesiaEffects0.000description1
- 238000013459approachMethods0.000description1
- 230000002146bilateral effectEffects0.000description1
- 230000015572biosynthetic processEffects0.000description1
- 230000010072bone remodelingEffects0.000description1
- GPRBEKHLDVQUJE-VINNURBNSA-NcefotaximeChemical compoundN([C@@H]1C(N2C(=C(COC(C)=O)CS[C@@H]21)C(O)=O)=O)C(=O)/C(=N/OC)C1=CSC(N)=N1GPRBEKHLDVQUJE-VINNURBNSA-N0.000description1
- 229960004261cefotaximeDrugs0.000description1
- 210000004513dentitionAnatomy0.000description1
- 238000011161developmentMethods0.000description1
- 230000018109developmental processEffects0.000description1
- 238000003745diagnosisMethods0.000description1
- 229940079593drugDrugs0.000description1
- 230000008030eliminationEffects0.000description1
- 238000003379elimination reactionMethods0.000description1
- 230000002349favourable effectEffects0.000description1
- 230000035876healingEffects0.000description1
- 230000001969hypertrophic effectEffects0.000description1
- 230000001771impaired effectEffects0.000description1
- 238000001802infusionMethods0.000description1
- 208000014674injuryDiseases0.000description1
- 239000000463materialSubstances0.000description1
- 230000035764nutritionEffects0.000description1
- 235000016709nutritionNutrition0.000description1
- 201000008482osteoarthritisDiseases0.000description1
- 230000009894physiological stressEffects0.000description1
- 238000004321preservationMethods0.000description1
- 230000002035prolonged effectEffects0.000description1
- 230000008707rearrangementEffects0.000description1
- 230000000717retained effectEffects0.000description1
- 230000000250revascularizationEffects0.000description1
- 230000033764rhythmic processEffects0.000description1
- 238000002560therapeutic procedureMethods0.000description1
- 230000036346tooth eruptionEffects0.000description1
- 230000008733traumaEffects0.000description1
Images

Landscapes
- Surgical Instruments (AREA)
- Prostheses (AREA)
Abstract
Description
Translated fromRussianИзобретение относится к медицине, а именно детской челюстно-лицевой хирургии, и может быть использовано при лечении детей с одно- или двусторонним анкилозом височно-нижнечелюстного сустава (ВНЧС), сопровождающимся нижней микрогнатией.The invention relates to medicine, namely, pediatric maxillofacial surgery, and can be used in the treatment of children with single or bilateral ankylosis of the temporomandibular joint (TMJ), accompanied by lower micrognatia.
Известен способ лечения анкилоза ВНЧС и нижней микрогнатии у детей с использованием аллогенного трансплантата (Котов Г.А., Семенов М.Г., Сафонов А.И. Применение аллогенной костной ткани при лечении детей с аномалиями развития челюстно-лицевой области. // Вiсник стоматологii. - 1999. - №1. - С.26-28).A known method of treating ankylosis of TMJ and lower micrognathia in children using an allogeneic transplant (Kotov G.A., Semenov M.G., Safonov A.I. Application of allogeneic bone tissue in the treatment of children with anomalies of the development of the maxillofacial region. // Visnik Dentist ii. - 1999. - No. 1. - S.26-28).
Однако аллогенный трансплантат не обладает достаточными пластическими свойствами, часто вызывает гнойно-воспалительные осложнения, редки случаи его перестройки в органотипичную кость.However, an allogeneic transplant does not have sufficient plastic properties, often causes purulent-inflammatory complications, and cases of its rearrangement into an organotypic bone are rare.
Известен способ лечения анкилоза ВНЧС и нижней микрогнатии у детей с использованием аутогенного костного трансплантата (Рогинский В.В., Арсенина О.И., Рабухина Н.А. Комплексное лечение детей с врожденными и приобретенными деформациями нижней челюсти. // Стоматология. - 1998. - №4. - С.32-36). Способ также имеет ряд недостатков: травматичность забора костного трансплантата, несоответствие размера и формы костного трансплантата и замещаемого костного изъяна, резорбция трансплантата при использовании для восполнения концевого дефекта челюсти, проблема подбора соответствующего донорского участка при повторных оперативных вмешательствах.A known method of treating ankylosis of TMJ and lower micrognathia in children using an autologous bone graft (Roginsky V.V., Arsenina O.I., Rabukhina N.A. Comprehensive treatment of children with congenital and acquired deformities of the lower jaw. // Dentistry. - 1998 . - No. 4. - S.32-36). The method also has several disadvantages: the trauma of the bone graft collection, the mismatch of the size and shape of the bone graft and the replaceable bone defect, the graft resorption when used to make up for an end jaw defect, the problem of selecting the appropriate donor site during repeated surgeries.
Наиболее близким способом к заявляемому изобретению является способ лечения анкилоза ВНЧС и нижней микрогнатии у детей с использованием компрессионно-дистракционного остеосинтеза (Харьков Л.В., Коротченко Г.М. Применение метода компрессионно-дистракционного остеогенеза для лечения детей с вторичными деформирующими артрозами и анкилозами височно-нижнечелюстного сустава. // Материалы Х конференции челюстно-лицевых хирургов и стоматологов. - 24-26 мая 2005 г. - С.188-189), принятый за прототип. Удаляют костные разрастания, освобождая суставную ямку. Резецируют гипертрофированный венечный отросток с частью височной мышцы. Трансплантируют венечный отросток с частью височной мышцы в область суставной ямки. Фиксируют трансплантат компрессионно-дистракционным устройством к суставному концу ветви челюсти. Активацию аппарата начинают на 7-10 сутки после операции по 1 мм в сутки. Дистракцию проводят до достижения благоприятного зубочелюстного соотношения под рентгенологическим контролем. Период ретенции продолжают в течение 2-3 месяцев, после чего дистрактор снимают.The closest method to the claimed invention is a method of treating ankylosis of TMJ and lower micrognathia in children using compression-distraction osteosynthesis (Kharkov L.V., Korotchenko G.M. Application of compression-distraction osteogenesis for the treatment of children with secondary deforming arthrosis and ankylosis of the temporomandibular -mandibular joint. // Materials of the Xth conference of maxillofacial surgeons and dentists. - May 24-26, 2005 - P.188-189), adopted as a prototype. Remove bone growths, freeing the articular fossa. A hypertrophic coronoid process with a part of the temporal muscle is resected. A coronoid process with a part of the temporal muscle is transplanted into the articular fossa. The transplant is fixed with a compression-distraction device to the articular end of the jaw branch. Activation of the apparatus begins on 7-10 days after surgery, 1 mm per day. The distraction is carried out until a favorable dentition ratio is achieved under radiological control. The retention period is continued for 2-3 months, after which the distractor is removed.
Недостатки прототипа:The disadvantages of the prototype:
- использование свободного костно-мышечного трансплантата резецированного венечного отростка с участком височной мышцы не может обеспечить полноценного костеобразования при компрессионно-дистракционном остеосинтезе, так как при резекции полностью нарушается его питание, а время, необходимое для реваскуляризации и перестройки костной ткани, превышает латентный период (7-10 суток);- the use of a free musculoskeletal transplant of a resected coronoid process with a temporal muscle site cannot provide complete bone formation during compression-distraction osteosynthesis, as its nutrition is completely impaired during resection, and the time required for revascularization and bone remodeling exceeds the latent period (7 -10 days);
- получаемый при компрессионно-дистракционном остеосинтезе костный регенерат имеет малую толщину, равную поперечному сечению основания венечного отростка, и малоустойчив к действию функциональной нагрузки.- the bone regenerate obtained by compression-distraction osteosynthesis has a small thickness equal to the cross section of the base of the coronoid process and is unstable to the action of the functional load.
Изобретение направлено на создание способа лечения анкилоза ВНЧС и нижней микрогнатии у детей, обеспечивающего формирование полноценного костного регенерата достаточной для физиологической нагрузки толщины.The invention is directed to the creation of a method for the treatment of ankylosis of TMJ and lower micrognathia in children, which ensures the formation of a full-fledged bone regenerate of sufficient thickness for physiological loading.
Указанный технический результат при реализации изобретения достигается тем, что в известном способе лечения анкилоза ВНЧС и нижней микрогнатии у детей, включающем остеотомию ветви челюсти под костными разрастаниями и их удаление, резекцию венечного отростка, компрессионно-дистракционный остеосинтез, особенность заключается в том, что остеотомированную поверхность ветви челюсти закрывают аутогенным дерможировым трансплантатом, проводят остеотомию ветви челюсти на уровне нижнечелюстного отверстия, сохраняя фиксацию медиальной крыловидной мышцы к суставному фрагменту, а затем компрессионно-дистракционный остеосинтез ветви челюсти. Кроме того, дерможировой трансплантат берут из подвздошной области или области ягодичной складки.The specified technical result in the implementation of the invention is achieved by the fact that in the known method of treating ankylosis of TMJ and lower micrognathia in children, including osteotomy of the jaw branch under bone growths and their removal, resection of the coronoid process, compression-distraction osteosynthesis, the peculiarity is that the osteotomy surface the jaw branches are closed with an autogenous dermal graft, an osteotomy of the jaw branch is performed at the level of the mandibular foramen, while maintaining fixation of the medial wing ovoid muscle to the articular fragment, and then compression-distraction osteosynthesis of the jaw branch. In addition, a dermal graft is taken from the iliac region or the gluteal fold.
Проведение линии остеотомии на уровне нижнечелюстного отверстия позволяет сохранить прикрепление верхних пучков медиальной крыловидной мышцы к суставному фрагменту ветви челюсти, увеличить объем костного регенерата при компрессионно-дистракционном остеосинтезе.Drawing a line of osteotomy at the level of the mandibular foramen allows maintaining the attachment of the upper bundles of the medial pterygoid muscle to the articular fragment of the jaw branch, and increasing the volume of bone regenerate during compression-distraction osteosynthesis.
Сохранение фиксации медиальной крыловидной мышцы к суставному фрагменту ветви челюсти обеспечивает его кровоснабжение, что является необходимым условием для получения полноценного костного регенерата при компрессионно-дистракционном остеосинтезе.Preservation of fixation of the medial pterygoid muscle to the articular fragment of the jaw branch ensures its blood supply, which is a necessary condition for obtaining a complete bone regenerate during compression-distraction osteosynthesis.
Увеличение объема костного регенерата ведет к увеличению его прочности и устойчивости к физиологической нагрузке.An increase in the volume of bone regenerate leads to an increase in its strength and resistance to physiological stress.
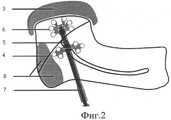
Способ осуществляется следующим образом (Фиг.1-3). Из подчелюстного доступа поднадкостнично обнажают наружную и заднюю поверхности ветви нижней челюсти, оставляя прикрепленной медиальную крыловидную мышцу. Бором и остеотомами проводят остеотомию ветви челюсти непосредственно под костными разрастаниями, которые частично или полностью удаляют (поз.1). Проводят удаление гипертрофированного венечного отростка (поз.2). При этом нижняя челюсть становится максимально подвижной. Из подвздошной области или области ягодичной складки берут деэпидермизированный дерможировой трансплантат (поз.3) с таким расчетом, чтобы он мог полностью закрыть остеотомированную поверхность ветви челюсти наподобие "шапочки". Донорскую рану послойно ушивают. Полученный трансплантат фиксируют к ветви челюсти нитью длительного рассасывания (более 30 суток) через 2 дополнительных отверстия по переднему и заднему краям. Проводят остеотомию ветви челюсти (поз.4) на уровне нижнечелюстного отверстия (поз.5), сохраняя фиксацию медиальной крыловидной мышцы, устанавливают компрессионно-дистракционное устройство (поз.7) для ветви нижней челюсти и фиксируют винтами (не менее 3-х на каждый фрагмент). Проводят компрессию отломков. Рану послойно зашивают.The method is as follows (Fig.1-3). From the submandibular approach, the external and posterior surfaces of the branches of the lower jaw are exposed subperiosteally, leaving the medial pterygoid muscle attached. Boron and osteotomes perform an osteotomy of the jaw branch directly under the bone growths, which are partially or completely removed (item 1). The hypertrophied coronoid process is removed (item 2). In this case, the lower jaw becomes as mobile as possible. From the iliac region or the region of the gluteal fold, a de-epidermal dermal transplant (pos. 3) is taken so that it can completely cover the osteotomized surface of the jaw branch like a “cap”. The donor wound is sutured in layers. The resulting graft is fixed to the jaw branch with a thread of prolonged resorption (more than 30 days) through 2 additional holes along the front and rear edges. An osteotomy of the jaw branch (item 4) is performed at the level of the mandibular foramen (item 5), while retaining the fixation of the medial pterygoid muscle, a compression-distraction device (item 7) is installed for the branch of the lower jaw and fixed with screws (at least 3 for each fragment). Fragments are compressed. The wound is sutured in layers.
Дистракцию начинают на 7-10 сутки после операции по 1 мм в сутки с ритмом 0,25 мм × 4 раза в день и продолжают до получения необходимого размера (поз.9). Ретенционный период составляет двойной период дистракции, по окончании которого устройство удаляют.Distraction begins on the 7-10th day after the operation, 1 mm per day with a rhythm of 0.25 mm × 4 times a day and continues until the desired size is obtained (pos. 9). The retention period is a double period of distraction, at the end of which the device is removed.
С возрастом при нарастании признаков нижней микрогнатии проводят повторный компрессионно-дистракционный остеосинтез ветви челюсти.With age, with an increase in signs of lower micrognathia, repeated compression-distraction osteosynthesis of the jaw branch is performed.
Заявляемый способ разработан и прошел клинические испытания у 6 пациентов, из них у 2-х больных с 2-х сторон. Получены хорошие функциональные и эстетические результаты в сроки наблюдения до 2 лет. Рецидивов анкилоза не наблюдалось, у всех больных устранена одно- или двусторонняя нижняя микрогнатия.The inventive method is developed and passed clinical trials in 6 patients, of which 2 patients from 2 sides. Good functional and aesthetic results were obtained in follow-up periods of up to 2 years. No relapse of ankylosis was observed; in all patients, one- or two-sided lower micrognathia was eliminated.
Приводим пример.We give an example.
Выписка из и/б №12967. Больной А. 3-х лет находился в клинике челюстно-лицевой хирургии ДГБ №19 с 17.04.06 по 27.04.06.Extract from / b No. 12967. Patient A. 3 years old was in the clinic of maxillofacial surgery, Children's hospital No 19 from 04/17/06 to 04/27/06.
Диагноз: анкилоз височно-нижнечелюстного сустава слева, нижняя микрогнатия слева.Diagnosis: ankylosis of the temporomandibular joint on the left, lower micrognathia on the left.
Операция: 18.04.06 устранение анкилоза ВНЧС и нижней микрогнатии слева: из подчелюстного доступа слева обнажены наружная и задняя поверхности ветви нижней челюсти, прикрепление медиальной крыловидной мышцы сохранено. Бором и остеотомом удалены костные разрастания и венечный отросток, нижняя челюсть мобилизована. Из правой подвздошной области взят деэпидермизированный дерможировой лоскут. Остеотомированные поверхности ветви челюсти укрыты лоскутом, который был фиксирован нитью Викрил 3/0. Проведена остеотомия ветви челюсти на уровне нижнечелюстного отверстия, сохранена фиксация верхних пучков медиальной крыловидной мышцы к суставному фрагменту, Фиг.1-3 (поз.6, 8), установлено и фиксировано шестью костными винтами малое накостное компрессионно-дистракционное устройство для ветви нижней челюсти фирмы "КОНМЕТ". Рана ушита послойно кетгутом и Этиленом 5/0. Донорская рана ушита послойно кетгутом и шелком 4/0.Operation: 04/18/06 elimination of ankylosis of TMJ and lower micrognathia on the left: from the submandibular access on the left, the external and posterior surfaces of the branches of the lower jaw are exposed, the attachment of the medial pterygoid muscle is preserved. Bone growths and the coronoid process were removed with a boron and osteotome, the lower jaw was mobilized. From the right iliac region, a de-epidermized dermirous flap was taken. Osteotomized surfaces of the jaw branch are covered with a flap that was fixed with Vikril 3/0 thread. An osteotomy of the jaw branch at the level of the mandibular foramen was performed, the fixation of the upper bundles of the medial pterygoid muscle to the articular fragment was retained, Figs. 1-3 (pos. 6, 8), a small osseous compression-distraction device for the lower jaw branch of the firm was installed and fixed with six bone screws "CONMET". The wound was sutured in layers catgut and
Медикаментозное лечение: цефотаксим 750 т × 3 р/д в/м курсом 6 дней, интра- и постоперационная инфузионная терапия, поливитамины.Drug treatment: cefotaxime 750 t × 3 r / d i / m for 6 days, intra- and postoperative infusion therapy, multivitamins.
Постоперационные раны зажили первичным натяжением, швы сняты на 7-10 сутки. Дистракция с 10-х суток по 0.25×4 р/д. Величина дистракции составила 20 мм, период ретенции 40 суток.Postoperative wounds healed by first intention, the sutures were removed on the 7-10th day. Distraction from 10 days to 0.25 × 4 p / d. The magnitude of the distraction was 20 mm, the retention period of 40 days.
11.07.06. под эндотрахеальным наркозом удалено компрессионно-дистракционное устройство. Заживление раны первичным натяжением.07/11/06. under endotracheal anesthesia removed compression-distraction device. Healing by first intention.
В результате проведенного лечения устранен анкилоз височно-нижнечелюстного сустава, открывание рта до 3,5 см, подбородок занимает срединное положение, устранена дизокклюзия.As a result of the treatment, ankylosis of the temporomandibular joint was eliminated, mouth opening up to 3.5 cm, the chin was in the middle position, disocclusion was eliminated.
Использование заявляемого способа позволяет:Using the proposed method allows you to:
- увеличить объем костного регенерата за счет остеотомии ветви челюсти на уровне нижнечелюстного отверстия;- increase the volume of bone regenerate due to osteotomy of the jaw branch at the level of the mandibular foramen;
- увеличить прочность костного регенерата за счет увеличения его объема;- increase the strength of bone regenerate by increasing its volume;
- получить полноценный костный регенерат в области укороченной ветви нижней челюсти на стороне анкилоза ВНЧС, так как сохраняется питание суставного фрагмента за счет медиальной крыловидной мышцы, а остеотомированная поверхность ветви закрывается дерможировым трансплантатом.- to obtain a full-fledged bone regenerate in the region of a shortened branch of the lower jaw on the side of the TMJ ankylosis, since the articular fragment is preserved due to the medial pterygoid muscle, and the osteotomized surface of the branch is closed by a dermiric graft.
Claims (2)
Translated fromRussianPriority Applications (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| RU2006144517/14ARU2334481C1 (en) | 2006-12-13 | 2006-12-13 | Method for treatment of temporomandibular joint ankylose and lower micrognathia in children |
Applications Claiming Priority (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| RU2006144517/14ARU2334481C1 (en) | 2006-12-13 | 2006-12-13 | Method for treatment of temporomandibular joint ankylose and lower micrognathia in children |
Publications (2)
| Publication Number | Publication Date |
|---|---|
| RU2006144517A RU2006144517A (en) | 2008-06-20 |
| RU2334481C1true RU2334481C1 (en) | 2008-09-27 |
Family
ID=39928840
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| RU2006144517/14ARU2334481C1 (en) | 2006-12-13 | 2006-12-13 | Method for treatment of temporomandibular joint ankylose and lower micrognathia in children |
Country Status (1)
| Country | Link |
|---|---|
| RU (1) | RU2334481C1 (en) |
Cited By (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2674116C1 (en)* | 2018-03-29 | 2018-12-04 | Общество с ограниченной ответственностью "Центр комплексной стоматологии" | Method of rehabilitation of children with anchylosis of temporomandibular joint and mandibular contractures in postoperative period |
| RU2699000C1 (en)* | 2018-05-08 | 2019-09-02 | Государственное Бюджетное учреждение здравоохранения города Москвы "Детская городская клиническая больница святого Владимира Департамента здравоохранения города Москвы" | Method for elimination of ankylosing injures of temporomandibular joint |
Citations (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2146894C1 (en)* | 1998-07-14 | 2000-03-27 | Иркутский государственный медицинский университет | Treatment method of inflammatory processes, osteoarthroses and ankyloses of temporomandibular articulation in children |
- 2006
- 2006-12-13RURU2006144517/14Apatent/RU2334481C1/ennot_activeIP Right Cessation
Patent Citations (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2146894C1 (en)* | 1998-07-14 | 2000-03-27 | Иркутский государственный медицинский университет | Treatment method of inflammatory processes, osteoarthroses and ankyloses of temporomandibular articulation in children |
Non-Patent Citations (2)
| Title |
|---|
| RAO К. The role of simultaneous gap arthroplasty and distraction osteogenesis in the management of temporo-mandibular joint ankylosis with mandibular deformity in children. J. Craniomaxillofac Surg. 2004 Feb; 32(1):38-42 (Adstract).* |
| Анкилоз височно-нижнечелюстного сустава. [ON-LINE], 06.11.2006, [найдено 24.10.2007], http://www.medicina.kharkov.ua/medref/ankiloz_2.html.* |
Cited By (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2674116C1 (en)* | 2018-03-29 | 2018-12-04 | Общество с ограниченной ответственностью "Центр комплексной стоматологии" | Method of rehabilitation of children with anchylosis of temporomandibular joint and mandibular contractures in postoperative period |
| RU2699000C1 (en)* | 2018-05-08 | 2019-09-02 | Государственное Бюджетное учреждение здравоохранения города Москвы "Детская городская клиническая больница святого Владимира Департамента здравоохранения города Москвы" | Method for elimination of ankylosing injures of temporomandibular joint |
Also Published As
| Publication number | Publication date |
|---|---|
| RU2006144517A (en) | 2008-06-20 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| Herford | Use of a plate-guided distraction device for transport distraction osteogenesis of the mandible | |
| McCarthy et al. | Distraction osteogenesis of the mandible: a ten-year experience | |
| Sawaki et al. | Mandibular lengthening by intraoral distraction using osseointegrated implants. | |
| Wells | Mandibular reconstruction using vascularized bone grafts | |
| Spinelli et al. | Surgical management of ankyloses of the temporomandibular joint by a piezoelectric device | |
| Rachmiel et al. | Extraoral vs. intraoral distraction osteogenesis in the treatment of hemifacial microsomia | |
| Tarng et al. | Management of bone defects due to infected non-union or chronic osteomyelitis with autologous non-vascularized free fibular grafts | |
| Siciliano et al. | Distraction osteogenesis of a fibula free flap used for mandibular reconstruction: preliminary report | |
| Troulis et al. | Distraction osteogenesis: Past, present, and future | |
| Chaudhary et al. | Open intercondylar fractures of the distal humerus: management using a mini–external fixator construct | |
| Li et al. | Reconstruction of mandibular symphyseal defects by trifocal distraction osteogenesis: an experimental study in Rhesus | |
| RU2456945C2 (en) | Method of eliminating defect of alveolar process of jaw | |
| Kildal et al. | Free vascularized bone grafts for reconstruction of traumatic bony defects of mandible and maxilla | |
| Hashemi et al. | Comparison between interpositional bone grafting and osteogenic alveolar distraction in alveolar bone reconstruction | |
| Wennogle et al. | A pin-in-groove technique for reduction of displaced subcondylar fractures of the mandible | |
| RU2334481C1 (en) | Method for treatment of temporomandibular joint ankylose and lower micrognathia in children | |
| Walker | Mandibular distraction osteogenesis for endosseous dental implants | |
| Zwetyenga et al. | Reconstruction of large mandibular and surrounding soft-tissue defects using distraction with bone transport | |
| RU2206287C2 (en) | Method for reconstruction of brachial distal department at incorrectly healed and unhealed intra-articular fractures | |
| Wu | Reaming bone grafting to treat tibial shaft aseptic nonunion after plating | |
| RU2625783C1 (en) | Method of taking the autotransplant from the cranks of the subdival bone | |
| Siavashi et al. | Evaluating the effect of double plating fixation with bone graft in nonunion of femoral and tibial fractures after primary surgery | |
| RU2797101C1 (en) | Method of removing limited jaw defects | |
| RU2668807C1 (en) | Method for abolition of cleft of upper alveolar ridge | |
| Feltsan et al. | Vertical distraction osteogenesis of frontal segment and platelet-rich plasma in the edentulous mandible |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| MM4A | The patent is invalid due to non-payment of fees | Effective date:20081214 |