RU2328229C1 - Method of similar intestinal continuity restoration - Google Patents
Method of similar intestinal continuity restorationDownload PDFInfo
- Publication number
- RU2328229C1 RU2328229C1RU2007116760/14ARU2007116760ARU2328229C1RU 2328229 C1RU2328229 C1RU 2328229C1RU 2007116760/14 ARU2007116760/14 ARU 2007116760/14ARU 2007116760 ARU2007116760 ARU 2007116760ARU 2328229 C1RU2328229 C1RU 2328229C1
- Authority
- RU
- Russia
- Prior art keywords
- anastomosis
- ligatures
- intestine
- suture
- edges
- Prior art date
Links
- 230000000968intestinal effectEffects0.000titleclaimsabstractdescription30
- 238000000034methodMethods0.000titleclaimsabstractdescription15
- 230000003872anastomosisEffects0.000claimsabstractdescription43
- 210000000936intestineAnatomy0.000claimsabstractdescription37
- 230000003886intestinal anastomosisEffects0.000claimsabstractdescription5
- 239000000834fixativeSubstances0.000claimsdescription18
- 210000001035gastrointestinal tractAnatomy0.000claims1
- 230000036770blood supplyEffects0.000abstractdescription4
- 238000001356surgical procedureMethods0.000abstractdescription3
- 239000003814drugSubstances0.000abstractdescription2
- 230000002123temporal effectEffects0.000abstract2
- 230000000694effectsEffects0.000abstract1
- 239000010410layerSubstances0.000abstract1
- 239000002356single layerSubstances0.000abstract1
- 239000000126substanceSubstances0.000abstract1
- 206010052428WoundDiseases0.000description17
- 208000027418Wounds and injuryDiseases0.000description17
- 210000001519tissueAnatomy0.000description11
- 210000002151serous membraneAnatomy0.000description7
- 210000004876tela submucosaAnatomy0.000description5
- 230000015572biosynthetic processEffects0.000description4
- 238000002347injectionMethods0.000description4
- 239000007924injectionSubstances0.000description4
- 210000000813small intestineAnatomy0.000description4
- 210000003815abdominal wallAnatomy0.000description3
- 230000001154acute effectEffects0.000description3
- 210000003205muscleAnatomy0.000description3
- 230000002980postoperative effectEffects0.000description3
- 206010016717FistulaDiseases0.000description2
- 241000270923Hesperostipa comataSpecies0.000description2
- 208000031481Pathologic ConstrictionDiseases0.000description2
- 210000003484anatomyAnatomy0.000description2
- 230000003890fistulaEffects0.000description2
- 238000002350laparotomyMethods0.000description2
- 239000000463materialSubstances0.000description2
- 210000004877mucosaAnatomy0.000description2
- 210000004400mucous membraneAnatomy0.000description2
- 230000003287optical effectEffects0.000description2
- 208000037804stenosisDiseases0.000description2
- 230000036262stenosisEffects0.000description2
- 230000002792vascularEffects0.000description2
- BQCIDUSAKPWEOX-UHFFFAOYSA-N1,1-DifluoroetheneChemical compoundFC(F)=CBQCIDUSAKPWEOX-UHFFFAOYSA-N0.000description1
- 206010007882CellulitisDiseases0.000description1
- 208000006784Cutaneous FistulaDiseases0.000description1
- 206010041899Stab woundDiseases0.000description1
- 210000001015abdomenAnatomy0.000description1
- 238000012084abdominal surgeryMethods0.000description1
- 230000006835compressionEffects0.000description1
- 238000007906compressionMethods0.000description1
- 238000002316cosmetic surgeryMethods0.000description1
- 238000003745diagnosisMethods0.000description1
- 208000037265diseases, disorders, signs and symptomsDiseases0.000description1
- 208000035475disorderDiseases0.000description1
- 230000002496gastric effectEffects0.000description1
- 230000035876healingEffects0.000description1
- 208000015181infectious diseaseDiseases0.000description1
- 230000000302ischemic effectEffects0.000description1
- 238000005399mechanical ventilationMethods0.000description1
- 210000000713mesenteryAnatomy0.000description1
- 230000002093peripheral effectEffects0.000description1
- 206010034674peritonitisDiseases0.000description1
- 238000002271resectionMethods0.000description1
- 231100000241scarToxicity0.000description1
- 238000004904shorteningMethods0.000description1
- 230000000472traumatic effectEffects0.000description1
Images







Landscapes
- Surgical Instruments (AREA)
Abstract
Description
Translated fromRussianПредлагаемое изобретение относится к медицине, а именно к абдоминальной хирургии, и может быть использовано для восстановления непрерывности одноименных отделов кишки после резекций, при пластических операциях, характеризующихся сложной конфигурацией линии кишечного шва, а также для создания обходных анастомозов в неоперабельных случаях.The present invention relates to medicine, namely to abdominal surgery, and can be used to restore the continuity of the same parts of the intestine after resections, plastic surgery, characterized by a complex configuration of the line of the intestinal suture, as well as to create bypass anastomoses in inoperable cases.
Осложнения со стороны анастомоза на любом уровне кишечной трубки чреваты тяжелыми последствиями и, нередко, смертью больного. Недостаточность анастомозов желудочно-кишечного тракта является причиной послеоперационного перитонита у 34-80% больных и в 40-60% случаев является причиной смерти (Егоров В.И. и соавт. Кишечные анастомозы. Физико-механические аспекты. - М.: Издательский дом Видар-М, 2004. - 304 с., ил.).Complications from the anastomosis at any level of the intestinal tube are fraught with serious consequences and, often, the death of the patient. Lack of gastrointestinal anastomoses is the cause of postoperative peritonitis in 34-80% of patients and in 40-60% of cases is the cause of death (Egorov V.I. et al. Intestinal anastomoses. Physico-mechanical aspects. - M.: Vidar Publishing House -M, 2004 .-- 304 p., Ill.).
Известен анастомоз по типу конец в конец, сформированный двухрядным швом Альберта (Островерхов Г.Е., Бомаш Ю.М., Лубоцкий Д.Н. Оперативная хирургия и топографическая анатомия. - Курск; Москва: АОЗТ «Литера», 1996 г. - 720 с., ил.), в нашей стране считается общепринятым (Островерхов Г.Е., Бомаш Ю.М., Лубоцкий Д.Н. Оперативная хирургия и топографическая анатомия. - Курск; Москва: АОЗТ «Литера», 1996 г. - 720 с., ил.; Егоров В.И. и соавт. Кишечные анастомозы. Физико-механические аспекты. - М.: Издательский дом Видар-М, 2004. - 304 с., ил.). Однако при сквозном прошивании кишечной стенки внутренним рядом швов возникает массивное инфицирование линии шва анастомоза. Второй, наружный ряд швов усугубляет нарушения ишемического характера в зоне анастомоза. Таким образом, создаются условия для заживления кишечной раны вторичным натяжением. Клинически состоятельные кишечные швы такого соустья в отдаленном послеоперационном периоде часто характеризуются грубым рубцом вплоть до стенозирования просвета соустья.Anastomosis of the end-to-end type is known, formed by a double-row Albert suture (Ostroverkhov G.E., Bomash Yu.M., Lubotsky D.N. Operative surgery and topographic anatomy. - Kursk; Moscow: AOZT Litera, 1996 - 720 pp., Ill.), In our country it is considered generally accepted (Ostroverkhov G.E., Bomash Yu.M., Lubotsky D.N. Surgical surgery and topographic anatomy. - Kursk; Moscow: CJSC Litera, 1996. - 720 p., Ill .; Egorov V.I. et al. Intestinal anastomoses. Physico-mechanical aspects. - M.: Vidar-M Publishing House, 2004. - 304 p., Ill.). However, with through flashing of the intestinal wall with the inner row of sutures, massive infection of the anastomotic suture line occurs. The second, outer row of sutures exacerbates ischemic disorders in the anastomotic zone. Thus, conditions are created for the healing of intestinal wounds by secondary intention. Clinically sound intestinal sutures of such an anastomosis in the distant postoperative period are often characterized by a rough scar up to stenosis of the lumen of the anastomosis.
В качестве ближайшего аналога принят «Способ кишечного шва» RU 02202293 С2, 20.03.2003, авторы Никитин Н.А., Касаткин Е.Н., Прокопьев Е.С., Бакулин П.С. Сущность изобретения заключается в краевом прошивании серозно-мышечно-подслизистого слоев каждой стенки кишечной раны в косом по отношению к поперечной оси кишки направлении параллельно боковым ветвям внутристеночных кишечных сосудов под углом, открытым в сторону брыжеечного края кишки. Вкол и выкол стежков на серозной оболочке каждого последующего шва производят на одной линии с выколом и вколом стежков на границе подслизистого и слизистого слоев предыдущего шва (фиг.1). Швы завязывают с формированием узлов на серозной оболочке.As the closest analogue adopted "Method of intestinal suture" RU 02202293 C2, 03.20.2003, authors Nikitin N.A., Kasatkin E.N., Prokopyev E.S., Bakulin P.S. The essence of the invention lies in the regional stitching of the serous-muscular-submucosal layers of each wall of the intestinal wound in an oblique direction with respect to the transverse axis of the intestine parallel to the lateral branches of the intraparietal intestinal vessels at an angle open to the mesenteric edge of the intestine. The injection and stitching of stitches on the serous membrane of each subsequent suture is performed in line with the stitching and injection of stitches at the border of the submucosal and mucous layers of the previous suture (Fig. 1). Sutures are tied with the formation of nodes on the serous membrane.
По сути, авторы предлагают способ наложения однорядного кишечного анастомоза по типу конец в конец. Однако шов может нарушать адекватное кровоснабжение в зоне кишечной раны по нескольким причинам:In fact, the authors propose a method for applying a single-row intestinal anastomosis of the end-to-end type. However, a suture may interfere with adequate blood supply in the intestinal wound for several reasons:
1. Обычно для формирования соустья используют зону, равноудаленную от двух прямых смежных краевых сосудов, где проходят сосуды четвертого и большего порядков, имеющие направление, параллельное продольной оси кишки, следовательно, швы в такой ситуации следует накладывать не под углом, а строго перпендикулярно поперечной оси кишки.1. Usually, for the formation of an anastomosis, a zone is used that is equidistant from two straight adjacent peripheral vessels where vessels of the fourth and greater orders pass, having a direction parallel to the longitudinal axis of the intestine, therefore, the sutures in this situation should not be laid at an angle, but strictly perpendicular to the transverse axis guts.
2. Предложенный способ шва не позволяет визуализировать сосуды подслизистой основы, что допускает возможность их прошивания.2. The proposed method of the suture does not allow to visualize the vessels of the submucosa, which allows the possibility of flashing them.
3. Накладывая швы под углом к поперечной оси кишки, авторы не учитывают принцип наикратчайшего расстояния. Таким образом, в момент затягивания шовная нить будет стремиться пройти расстояние между точками вкола и выкола на серозе, что должно привести к компрессии интрамуральных сосудов на участке между шовной нитью и краем кишки, даже если сосуды расположены параллельно ходу шовной нити.3. Suturing at an angle to the transverse axis of the intestine, the authors do not take into account the principle of shortest distance. Thus, at the time of tightening, the suture thread will tend to go the distance between the points of injection and puncture on serosa, which should lead to compression of the intramural vessels in the area between the suture thread and the intestinal edge, even if the vessels are parallel to the suture.
Также предложенный способ не гарантирует точного сопоставления одноименных тканей соустья.Also, the proposed method does not guarantee accurate matching of the same tissues of the anastomosis.
Задачи: обеспечение состоятельности соустья, сохранение адекватного кровоснабжения в зоне соустья, обеспечение точного сопоставления одноименных тканей соустья, предупреждение анастомозита, сокращение сроков лечения и пребывания в стационаре, а в целом сокращение сроков медико-социальной реабилитации.Tasks: ensuring the consistency of the anastomosis, maintaining adequate blood supply in the anastomosis zone, ensuring accurate matching of the anastomosis tissues of the same name, preventing anastomositis, shortening the treatment and hospital stay, and generally reducing the time of medical and social rehabilitation.
Технической новизной предлагаемого способа является то, что осуществляют пересечение кишки на середине расстояния между двумя прямыми смежными сосудами, затем дополнительно мобилизуют на двух временных фиксирующих лигатурах подслизистый слой острым путем на протяжении 5-6 мм, снимают временные фиксирующие лигатуры с брыжеечного края каждой культи кишки и накладывают первый шов, а противобрыжеечные временные фиксирующие лигатуры разводят в стороны до образования прямого угла между ними и равномерно натягивают, со стороны брыжеечного края накладывают очередной шов при условии полного расправления тканей в каждом межшовном промежутке, временные фиксирующие лигатуры сближают, предыдущий шов завязывают, затем временные фиксирующие лигатуры вновь разводят и последовательно повторяют манипуляции до наложения шва на противобрыжеечном краю кишки, таким образом, швы накладывают попарно и завязывают строго последовательно, при этом каждый последующий шов является сопоставляющим для предыдущего, далее временные фиксирующие лигатуры снимают, после чего кишку ротируют на 180 градусов вдоль продольной ее оси за угловые швы и моделируют геометрию раневой апертуры анастомоза в виде ромба с помощью двух временных фиксирующих лигатур, осуществляют последовательное наложение швов в условиях постепенного сведения краев кишечной раны подобным образом.The technical novelty of the proposed method is that the intestine is crossed at the middle of the distance between two direct adjacent vessels, then the submucous layer is additionally mobilized on two temporary fixative ligatures in the acute way for 5-6 mm, temporary fixative ligatures are removed from the mesenteric edge of each intestinal stump and the first suture is applied, and the anti-mesenteric temporary fixative ligatures are bred to the sides until a right angle is formed between them and evenly stretched from the mesenteric side the edges are sutured again under the condition of complete expansion of the tissues in each intersutomous gap, the temporary fixative ligatures are brought closer together, the previous suture is tied, then the temporary fixative ligatures are again diluted and the procedures are repeated until the suture is placed on the mesenteric edge of the intestine, thus, the sutures are applied in pairs and are tied strictly successively, with each subsequent suture being matching for the previous one, then the temporary fixative ligatures are removed, after which the intestine is rotated by 1 80 degrees along its longitudinal axis behind the fillet seams and model the geometry of the wound aperture of the anastomosis in the form of a rhombus using two temporary fixative ligatures; sequential suturing is performed under conditions of gradual reduction of the edges of the intestinal wound in a similar manner.
Для наглядности способ иллюстрирован фиг.1-8, на которых:For clarity, the method is illustrated in figures 1-8, in which:
1 - прямые смежные сосуды;1 - direct adjacent vessels;
2 - сосуд четвертого порядка;2 - a vessel of the fourth order;
3 - серозно-мышечный футляр;3 - serous-muscular case;
4 - слизисто-подслизистый футляр;4 - mucous-submucous case;
5 - временная фиксирующая лигатура 1;5 - temporary
6 - временная фиксирующая лигатура 2;6 - temporary
7 - угловой шов 1;7 -
8 - серозная оболочка;8 - serous membrane;
9 - мышечный слой;9 - muscle layer;
10 - подслизистая основа;10 - submucosa;
11 - собственно слизистая;11 - the actual mucosa;
12 - шовная нить;12 - suture thread;
13 - угловой шов 2;13 -
14 - временные фиксирующие лигатуры 3, 4.14 -
Способ осуществляют следующим образом.The method is as follows.
Пересечение кишки осуществляют на середине расстояния между двумя прямыми 1 смежными сосудами, т.е. в области внутристеночных сосудов четвертого порядка 2, имеющих ход, параллельный продольной оси кишки. При пересечении кишки серозно-мышечный футляр 3 и слизисто-подслизистый футляр 4 расходятся в стороны приблизительно в равной степени, что в известной мере открывает последний (фиг.1). Слизисто-подслизистый футляр прошивают по брыжеечному и противобрыжеечному краям двумя временными фиксирующими лигатурами 5, 6 и в условиях умеренного их натяжения мобилизуют подслизистый слой острым путем (иссечением краевой полоски серозно-мышечного футляра) на протяжении 5-6 мм. Как правило, это достаточное расстояние для визуализации сосудов подслизистой основы. Такая мобилизация позволит проводить иглу в области сосудов четвертого порядка (фиг.2) параллельно их ходу. Аналогичным образом обрабатывают вторую культю анаотомозируемой кишки.Intestine intersection is carried out in the middle of the distance between two
Накладывают угловой шов 7 на брыжеечные края анастомозируемых отрезков кишки и временные фиксирующие лигатуры 6 на противобрыжеечные края кишки. С помощью этих нитей создают геометрию раневой апертуры анастомоза в виде равнобедренного треугольника с углом вершины не менее 90 градусов (фиг.3), роль катетов которого будут выполнять мобилизованные края кишки, а основанием (гипотенуза) выступит гипотетическая линия, соединяющая противобрыжеечные края дистальной и проксимальной культи кишки.Impose an
Данный технический прием оправдан следующими причинами:This technique is justified by the following reasons:
- угол 90 и более градусов позволяет проводить иглу в тканях одной культи кишки без риска случайного захвата другой культи;- an angle of 90 or more degrees allows you to hold the needle in the tissues of one stump of the intestine without the risk of accidentally capturing another stump;
- равные катеты раневой апертуры резко снижают риск гофрирования анастомоза;- equal legs of the wound aperture sharply reduce the risk of corrugation of the anastomosis;
- максимальное расправление тканей в каждом межшовном промежутке полностью исключает возможность развития стеноза соустья.- the maximum expansion of the tissues in each intershoot completely eliminates the possibility of developing stenosis of the anastomosis.
- манипулируя держалками (натягиваем перед прошиванием, выявляя сосудистую архитектуру подслизистой основы и погружая слизистую в просвет; сближаем во время затягивания нити, уменьшая натяжение в тканях) оптимизируем процесс наложения анастомоза.- by manipulating the holders (we tighten before flashing, revealing the vascular architecture of the submucosa and immersing the mucosa into the lumen; we bring it together while tightening the threads, reducing the tension in the tissues) we optimize the process of applying the anastomosis.
Вкол иглы производят со стороны серозной оболочки 8 на расстоянии 5 мм от края серозно-мышечного футляра. Проводят иглу с нитью 12 через мышцы 9 и всю толщу подслизистой основы 10, выкалывают на ее краю, не захватывая собственно слизистую 11. Иглу и нить проводят строго параллельно продольной оси кишки и, соответственно, параллельно ходу сосудов подслизистого слоя. На втором анастомозируемом участке кишки повторяют ход иглы в обратном порядке с выколом ее на серозной оболочке в 0,5 см от края наружного футляра (фиг.4). Проведение иглы в тканях производят под контролем трехкратного оптического увеличения.The needle is injected from the side of the serous membrane 8 at a distance of 5 mm from the edge of the serous-muscular case. A needle with a
Швы затягивают после сближения краев анастомозируемых концов кишки, строго последовательно, при этом каждый последующий шов является сопоставляющим для предыдущего. Это означает, что швы накладывают попарно, не завязывая их, а затем последний шов натягивают, сопоставляя края анастомоза, а предыдущий, в условиях точно сопоставленных краев соустья, завязывают. Далее накладывают следующий шов, выполняющий роль сопоставляющего, и так далее (прием двух парных «шагающих» швов). Это позволяет достигнуть точного сопоставления слоев кишечной стенки в соустье и избежать избыточного натяжения в тканях под завязываемой шовной нитью.The sutures are tightened after the edges of the anastomosed ends of the intestine come together, strictly sequentially, with each subsequent suture being comparable for the previous one. This means that the sutures are applied in pairs without tying them, and then the last suture is pulled, comparing the edges of the anastomosis, and the previous one, in conditions of precisely matched edges of the anastomosis, is tied. Next, impose the next seam, performing the role of matching, and so on (the reception of two paired "walking" seams). This allows you to achieve an exact comparison of the layers of the intestinal wall in the anastomosis and to avoid excessive tension in the tissues under the knotted suture thread.
Таким образом, наложение швов при формировании анастомоза производят в условиях динамического моделирования формы кишечной раны, создавая угол около 90 градусов между краями раны в момент прошивания слоев кишечной стенки (фиг.5) и сближая край кишечной раны при завязывании узла (фиг.6).Thus, suturing during the formation of the anastomosis is performed under conditions of dynamic modeling of the shape of the intestinal wound, creating an angle of about 90 degrees between the edges of the wound at the time of suturing the layers of the intestinal wall (Fig. 5) and bringing the edge of the intestinal wound closer when tying the knot (Fig. 6).
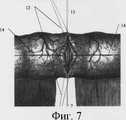
Наложение швов на противоположную полуокружность анастомоза осуществляют в условиях ротации кишки на 180° вдоль продольной оси за угловые швы 7, 13. На середину расстояния между брыжеечным и противобрыжеечным краями обоих анастомозируемых концов кишки накладывают временные фиксирующие лигатуры 14, с помощью которых моделируют геометрию раневой апертуры анастомоза в виде ромба (фиг.7). Наложение швов осуществляют вышеописанным способом, завязывание их также производят последовательно в условиях сведения краев кишечной раны. Последние 4-5 швов анастомоза накладывают не завязывая (фиг.8) с целью визуального контроля прохождения иглы через слои кишечной стенки, а затем последовательно завязывают предварительно наложенные швы. Таким образом, также реализуют принцип динамического моделирования формы кишечной раны в процессе формирования анастомоза.Suturing of the opposite semicircle of the anastomosis is carried out under conditions of intestinal rotation 180 ° along the longitudinal axis behind the
Расстояние между швами не является строго фиксированным, в первую очередь учитывают сосудистый рисунок подслизистой основы. Для шва используют синтетический монофиламентный материал на атравматических иглах условным номером 5/0-6/0. Количество петель в узле делают не менее четырех, пространственное строение их - параллельное или смешанное.The distance between the sutures is not strictly fixed, primarily the vascular pattern of the submucosa is taken into account. For the suture, synthetic monofilament material is used on atraumatic needles with the
Клинический пример:Clinical example:
Больной Б., 47 лет, находился на стационарном лечении в первом хирургическом отделении РЦФХГ с 12.10.06. по 24.10,06 г. Поступил с жалобами на наличие длительно незаживающего свища тонкой кишки в правой боковой области, повышение температуры до 38 градусов. Из анамнеза: оперирован 5 месяцев назад в районной больнице по поводу множественных колото-резанных ран живота (выполнена лапаротомия, ушивание поврежденной тонкой кишки). На основании проведенного исследования был установлен диагноз: Высокий наружный губовидный длительно незаживающий свищ тонкой кишки травматического генеза. Флегмона передней брюшной стенки в области устья свищевого хода. Больной оперирован: произведена срединная лапаротомия (ТВА + ИВЛ), выделен патологически измененный участок тонкой кишки, и резицирован в области сосудов четвертого порядка. Слизисто-подслизистый футляр прошили по брыжеечному и противобрыжеечному краям двумя временными фиксирующими лигатурами и в условиях умеренного их натяжения мобилизовали подслизистый слой острым на протяжении 5-6 мм. Аналогичным образом обработали вторую культю анастомозируемой кишки.Patient B., 47 years old, was hospitalized in the first surgical department of RCSCH from 10/12/06. on 10.24.06. Received with complaints of the presence of a long nonhealing fistula of the small intestine in the right lateral region, an increase in temperature to 38 degrees. From the anamnesis: operated 5 months ago in a district hospital for multiple stab wounds of the abdomen (performed laparotomy, suturing of the damaged small intestine). On the basis of the study, the diagnosis was established: High external labiform long-unhealed fistula of the small intestine of traumatic origin. Phlegmon of the anterior abdominal wall in the area of the mouth of the fistulous passage. The patient was operated on: a median laparotomy (TBA + mechanical ventilation) was performed, a pathologically changed part of the small intestine was isolated, and resected in the region of fourth-order vessels. The mucous-submucosal case was stitched along the mesenteric and anti-mesenteric edges with two temporary fixative ligatures and under moderate tension they mobilized the submucosal layer acute for 5-6 mm. The second stump of the anastomosed intestine was similarly treated.
Наложили угловой шов на брыжеечные края анастомозируемых отрезков кишки и временные фиксирующие лигатуры на противобрыжеечные края кишки. С помощью этих нитей создали геометрию раневой апертуры анастомоза в виде равнобедренного треугольника с углом вершины не менее 90 градусов. Далее со стороны серозной оболочки произвели вкол на расстоянии 5 мм от края серозно-мышечного футляра. Проведя иглу с нитью через мышцы и всю толщу подслизистой основы, выкалывали на ее краю, не захватывая собственно слизистую. Иглу и нить проводили строго параллельно продольной оси кишки и, соответственно, параллельно ходу сосудов подслизистого слоя. На втором анастомозируемом участке кишки повторяли ход иглы в обратном порядке с выколом ее на серозной оболочке в 5 мм от края наружного футляра. Проведение иглы в тканях производили под контролем трехкратного оптического увеличения.An angular suture was placed on the mesenteric edges of the anastomosed segments of the intestine and temporary fixative ligatures on the anti-mesenteric edges of the intestine. Using these threads, the geometry of the wound aperture of the anastomosis was created in the form of an isosceles triangle with an apex angle of at least 90 degrees. Further, an injection was made from the side of the serous membrane at a distance of 5 mm from the edge of the serous-muscular case. After passing a needle with a thread through the muscles and the entire thickness of the submucosal base, they were punctured on its edge, without capturing the mucous membrane itself. The needle and thread were carried out strictly parallel to the longitudinal axis of the intestine and, accordingly, parallel to the course of the vessels of the submucosal layer. On the second anastomotic section of the intestine, the needle was repeated in the reverse order with its puncture on the
Швы затягивали после сближения краев анастомозируемых концов кишки, строго последовательно, при этом каждый последующий шов являлся сопоставляющим для предыдущего. Это означает, что швы накладывали попарно, не завязывая их, а затем последний шов натягивали, сопоставляя края анастомоза, а предыдущий, в условиях точно сопоставленных краев соустья, завязывали. Далее накладывали следующий шов, выполняющий роль сопоставляющего, и так далее (прием двух парных «шагающих» швов). Это позволило достигнуть точного сопоставления слоев кишечной стенки в соустье и избежать избыточного натяжения в тканях под завязываемой шовной нитью.The sutures were tightened after the edges of the anastomosed ends of the intestine converged, strictly sequentially, with each subsequent suture being comparable for the previous one. This means that the sutures were applied in pairs without tying them, and then the last suture was pulled, comparing the edges of the anastomosis, and the previous one, in conditions of precisely matched edges of the anastomosis, was tied. Next, the next stitch was applied, acting as a matching one, and so on (the reception of two paired “walking” stitches). This made it possible to achieve an exact comparison of the layers of the intestinal wall in the anastomosis and to avoid excessive tension in the tissues under the knotted suture thread.
Наложение швов на противоположную полуокружность анастомоза осуществляли в условиях ротации кишки на 180° вдоль продольной оси за угловые швы. На середину расстояния между брыжеечным и противобрыжеечным краями обоих анастомозируемых концов кишки накладывали временные фиксирующие лигатуры, с помощью которых моделировали геометрию раневой апертуры анастомоза в виде ромба. Наложение швов осуществляли вышеописанным способом, завязывание их также производили последовательно в условиях сведения краев кишечной раны. Последние 4-5 швов анастомоза накладывали не завязывая, с целью визуального контроля прохождения иглы через слои кишечной стенки, а затем последовательно завязывали предварительно наложенные швы. Для шва использовали рассасывающийся синтетический монофиламентный материал на атравматических иглах условным номером 5/0-6/0 (PDS II). Окно в брыжейке ушито. Патологически измененный участок передней брюшной стенки иссечен, ушит. Послойное ушивание раны передней брюшной стенки по принятой в клинике методике. Обычное послеоперационное течение. Швы сняты на 10-е сутки. На 12-е сутки выписан из отделения в удовлетворительном состоянии.Suturing on the opposite semicircle of the anastomosis was carried out under conditions of intestinal rotation by 180 ° along the longitudinal axis behind the fillet seams. Temporary fixing ligatures were applied to the middle of the distance between the mesenteric and mesenteric edges of both anastomosed ends of the intestine, with the help of which the geometry of the wound aperture of the anastomosis in the form of a rhombus was simulated. Suturing was carried out as described above, they were also tied sequentially under conditions of reducing the edges of the intestinal wound. The last 4-5 sutures of the anastomosis were imposed without tying, in order to visually control the passage of the needle through the layers of the intestinal wall, and then the previously applied sutures were sequentially tied. For the suture, a resorbable synthetic monofilament material on atraumatic needles with the
Данным способом было прооперированно 17 больных с высокими наружными свищами. Несостоятельности анастомозов не было, что подтверждено рентгенологическими исследованиями. Средний койкодень составил 11 дней.In this way, 17 patients with high external fistulas were operated on. Anastomosis failure was not, as confirmed by x-ray studies. The average bed day was 11 days.
Использование способа позволяет обеспечить состоятельность соустья, сохранить адекватное кровоснабжение в зоне соустья, точно сопоставить одноименные ткани соустья встык, предупредить развитие анастомозита, сократить сроки лечения и пребывания в стационаре, а в целом сократить сроки медико-социальной реабилитации.Using the method allows to ensure the consistency of the anastomosis, maintain adequate blood supply in the anastomosis zone, accurately compare the same-name tissues of the anastomosis butt, prevent the development of anastomositis, reduce treatment and hospital stay, and generally reduce the time of medical and social rehabilitation.
Claims (1)
Translated fromRussianPriority Applications (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| RU2007116760/14ARU2328229C1 (en) | 2007-05-03 | 2007-05-03 | Method of similar intestinal continuity restoration |
Applications Claiming Priority (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| RU2007116760/14ARU2328229C1 (en) | 2007-05-03 | 2007-05-03 | Method of similar intestinal continuity restoration |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| RU2328229C1true RU2328229C1 (en) | 2008-07-10 |
Family
ID=39680611
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| RU2007116760/14ARU2328229C1 (en) | 2007-05-03 | 2007-05-03 | Method of similar intestinal continuity restoration |
Country Status (1)
| Country | Link |
|---|---|
| RU (1) | RU2328229C1 (en) |
Cited By (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2718281C1 (en)* | 2019-04-26 | 2020-04-01 | федеральное государственное автономное образовательное учреждение высшего образования Первый Московский государственный медицинский университет имени И.М. Сеченова Министерства здравоохранения Российской Федерации (Сеченовский университет) (ФГАОУ ВО Первый МГМУ им. И.М. Сеченова Минздрава России (Се | Method of continuous serous-muscular-submucous one-row intestinal suture with visual control along whole rectum circumference |
Citations (3)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2173103C1 (en)* | 2000-02-09 | 2001-09-10 | Оренбургская государственная медицинская академия | Method for performing entero-enteroanastomosis |
| RU2202293C2 (en)* | 1999-10-11 | 2003-04-20 | Гетманова Алла Викторовна | Method for applying intestinal suture |
| US6769594B2 (en)* | 2002-05-31 | 2004-08-03 | Tyco Healthcare Group, Lp | End-to-end anastomosis instrument and method for performing same |
- 2007
- 2007-05-03RURU2007116760/14Apatent/RU2328229C1/ennot_activeIP Right Cessation
Patent Citations (3)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2202293C2 (en)* | 1999-10-11 | 2003-04-20 | Гетманова Алла Викторовна | Method for applying intestinal suture |
| RU2173103C1 (en)* | 2000-02-09 | 2001-09-10 | Оренбургская государственная медицинская академия | Method for performing entero-enteroanastomosis |
| US6769594B2 (en)* | 2002-05-31 | 2004-08-03 | Tyco Healthcare Group, Lp | End-to-end anastomosis instrument and method for performing same |
Non-Patent Citations (1)
| Title |
|---|
| ЕГИЕВ В.Н. Однорядный непрерывный шов анастомозов в абдоминальной хирургии. - М.: Медпрактика-М, 2002, 80-83. SCHEELE J. et al. Effect of anastomosis technic on wound healing in the gastrointestinal tract, Z Exp Chir Transplant Kunstliche Organe, 1985, 18(6), 357-367.* |
Cited By (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2718281C1 (en)* | 2019-04-26 | 2020-04-01 | федеральное государственное автономное образовательное учреждение высшего образования Первый Московский государственный медицинский университет имени И.М. Сеченова Министерства здравоохранения Российской Федерации (Сеченовский университет) (ФГАОУ ВО Первый МГМУ им. И.М. Сеченова Минздрава России (Се | Method of continuous serous-muscular-submucous one-row intestinal suture with visual control along whole rectum circumference |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| Gai et al. | Pancreaticojejunostomy conducive to biological healing in minimally invasive pancreaticoduodenectomy | |
| RU2328229C1 (en) | Method of similar intestinal continuity restoration | |
| RU2432126C2 (en) | Method for creating pancreatojejunal anastomosis in proximal pancreatectomy | |
| RU2202293C2 (en) | Method for applying intestinal suture | |
| RU2698985C1 (en) | Method of manual continuous combined vascular suture for eliminating an inferior vena cava defect | |
| RU2530489C1 (en) | Method of e.r. timbakov's process of one-row intestinal suture | |
| RU2696656C1 (en) | Method of surgical treatment of duodenal ulcer | |
| RU2391055C2 (en) | Method of esophageal-enteric anastomoses formation at surgical treatment of cardioesophageal cancer | |
| RU2525732C1 (en) | Method of oesophageal hiatus plasty | |
| RU2689870C1 (en) | Method of forming intraocorporal laparoscopic term-terminal invagination and ileotransverse anastomosis | |
| RU2328992C1 (en) | Method of surgical formation of invaginated one-row large intestinal anastomosis | |
| RU2692463C2 (en) | Method for liver wounds closure | |
| RU2263472C2 (en) | Method for suturing in laparotomic wound due to formation of duplicature | |
| RU2535075C2 (en) | Method of forming end-side oesophageal-gastric anastomosis after proximal stomach resection | |
| RU2645116C2 (en) | Method for laparoscopic intracorporal manual gastroenteroanastomosis | |
| RU2143234C1 (en) | Methods of surgical treatment of esophagus achalasia | |
| RU2412657C1 (en) | Method of surgical management and prevention of recurrent hemopphages in oesophageal and cardia varicose veins dilatation | |
| RU2833760C1 (en) | Method for formation of oesophagogastroanastomosis after minimally invasive video-assisted thoracolaparoscopic resection of oesophagus of lewis type | |
| RU2341205C2 (en) | Method of formation of esophageal-intestinal anastomosis | |
| RU2726346C1 (en) | Side-to-side enteroenteroanastomosis protection and reinforcement method when using a linear suturing device | |
| RU2467707C1 (en) | Kravtsov's method skin flap formation in urethroplasty for proximal hypospadias | |
| RU2456943C1 (en) | Method of applying anastomosis between hollow organs of abdominal cavity | |
| RU2710215C1 (en) | Method for aseptic organ-preserving resection of hollow organs of the digestive tract | |
| RU2549016C1 (en) | Method for biliary repair in gautier's orthotopic transplantation of left lateral liver sector in children with transplant having common orifice of bile ducts of ii and iii liver segments | |
| RU2532383C1 (en) | Method for surgical approach to corrosive strictures of terminal portion of common bile duct |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| MM4A | The patent is invalid due to non-payment of fees | Effective date:20090504 |