RU2212194C1 - Draining unit for creating biliodigestive anastomosis - Google Patents
Draining unit for creating biliodigestive anastomosisDownload PDFInfo
- Publication number
- RU2212194C1 RU2212194C1RU2002104566/14ARU2002104566ARU2212194C1RU 2212194 C1RU2212194 C1RU 2212194C1RU 2002104566/14 ARU2002104566/14 ARU 2002104566/14ARU 2002104566 ARU2002104566 ARU 2002104566ARU 2212194 C1RU2212194 C1RU 2212194C1
- Authority
- RU
- Russia
- Prior art keywords
- drainage
- mushroom
- anastomosis
- lumen
- creating
- Prior art date
Links
- 230000003872anastomosisEffects0.000titleclaimsabstractdescription12
- 210000000056organAnatomy0.000claimsabstractdescription4
- 239000000463materialSubstances0.000claimsabstract2
- 235000001674Agaricus brunnescensNutrition0.000claimsdescription8
- 230000015572biosynthetic processEffects0.000claimsdescription5
- 210000001953common bile ductAnatomy0.000claimsdescription2
- 239000000126substanceSubstances0.000abstract1
- 206010061876ObstructionDiseases0.000description5
- 238000013508migrationMethods0.000description4
- 230000005012migrationEffects0.000description4
- 210000000232gallbladderAnatomy0.000description3
- 210000002784stomachAnatomy0.000description3
- HSINOMROUCMIEA-FGVHQWLLSA-N(2s,4r)-4-[(3r,5s,6r,7r,8s,9s,10s,13r,14s,17r)-6-ethyl-3,7-dihydroxy-10,13-dimethyl-2,3,4,5,6,7,8,9,11,12,14,15,16,17-tetradecahydro-1h-cyclopenta[a]phenanthren-17-yl]-2-methylpentanoic acidChemical compoundC([C@@]12C)C[C@@H](O)C[C@H]1[C@@H](CC)[C@@H](O)[C@@H]1[C@@H]2CC[C@]2(C)[C@@H]([C@H](C)C[C@H](C)C(O)=O)CC[C@H]21HSINOMROUCMIEA-FGVHQWLLSA-N0.000description2
- BPYKTIZUTYGOLE-IFADSCNNSA-NBilirubinChemical compoundN1C(=O)C(C)=C(C=C)\C1=C\C1=C(C)C(CCC(O)=O)=C(CC2=C(C(C)=C(\C=C/3C(=C(C=C)C(=O)N\3)C)N2)CCC(O)=O)N1BPYKTIZUTYGOLE-IFADSCNNSA-N0.000description2
- 102000009123FibrinHuman genes0.000description2
- 108010073385FibrinProteins0.000description2
- BWGVNKXGVNDBDI-UHFFFAOYSA-NFibrin monomerChemical compoundCNC(=O)CNC(=O)CNBWGVNKXGVNDBDI-UHFFFAOYSA-N0.000description2
- 239000003613bile acidSubstances0.000description2
- 210000000013bile ductAnatomy0.000description2
- 210000003445biliary tractAnatomy0.000description2
- 239000013078crystalSubstances0.000description2
- 229950003499fibrinDrugs0.000description2
- 235000013305foodNutrition0.000description2
- 230000002980postoperative effectEffects0.000description2
- 238000001356surgical procedureMethods0.000description2
- 206010023129Jaundice cholestaticDiseases0.000description1
- 206010028980NeoplasmDiseases0.000description1
- 201000005267Obstructive JaundiceDiseases0.000description1
- 208000002193PainDiseases0.000description1
- 206010061902Pancreatic neoplasmDiseases0.000description1
- XUIMIQQOPSSXEZ-UHFFFAOYSA-NSiliconChemical compound[Si]XUIMIQQOPSSXEZ-UHFFFAOYSA-N0.000description1
- 206010052428WoundDiseases0.000description1
- 208000027418Wounds and injuryDiseases0.000description1
- 210000000941bileAnatomy0.000description1
- 208000027119bilirubin metabolic diseaseDiseases0.000description1
- 238000009534blood testMethods0.000description1
- 208000003167cholangitisDiseases0.000description1
- 230000006835compressionEffects0.000description1
- 238000007906compressionMethods0.000description1
- 238000003745diagnosisMethods0.000description1
- 201000010099diseaseDiseases0.000description1
- 208000037265diseases, disorders, signs and symptomsDiseases0.000description1
- 239000003814drugSubstances0.000description1
- 210000001198duodenumAnatomy0.000description1
- 210000001035gastrointestinal tractAnatomy0.000description1
- 208000036796hyperbilirubinemiaDiseases0.000description1
- 210000000936intestineAnatomy0.000description1
- 208000015486malignant pancreatic neoplasmDiseases0.000description1
- 230000036407painEffects0.000description1
- 201000002528pancreatic cancerDiseases0.000description1
- 208000008443pancreatic carcinomaDiseases0.000description1
- 238000007458percutaneous transhepatic cholangiographyMethods0.000description1
- 229920001296polysiloxanePolymers0.000description1
- 229940121896radiopharmaceuticalDrugs0.000description1
- 239000012217radiopharmaceuticalSubstances0.000description1
- 230000002799radiopharmaceutical effectEffects0.000description1
- 238000010992refluxMethods0.000description1
- 229910052710siliconInorganic materials0.000description1
- 239000010703siliconSubstances0.000description1
- 238000002560therapeutic procedureMethods0.000description1
Images

Landscapes
- Surgical Instruments (AREA)
- External Artificial Organs (AREA)
Abstract
Description
Translated fromRussianИзобретение относится к медицине, а именно к хирургии, и может быть использовано для формирования билиодигестивных анастомозов с "потерянным" дренажом. The invention relates to medicine, namely to surgery, and can be used to form biliodigestive anastomoses with "lost" drainage.
Известны различные типы дренажей для формирования таких анастомозов. Известен дренаж для формирования анастомоза в виде однопросветной полой трубки с перфорационными отверстиями на ее концах (Е.В. Смирнов. Хирургические операции на желчных путях, Медгиз, 1961 г., с.103-113). Однако недостатком этих дренажей является возможность их миграции и утраты "каркасных" свойств в месте анастомоза. Various types of drains are known for the formation of such anastomoses. Known drainage for the formation of an anastomosis in the form of a single-lumen hollow tube with perforations at its ends (EV Smirnov. Surgical operations on the biliary tract, Medgiz, 1961, p.103-113). However, the disadvantage of these drains is the possibility of their migration and loss of "frame" properties at the site of the anastomosis.
Чтобы избежать миграции дренажа из желчных путей предложено устройство - дренаж с "грибовидными" расширениями на обоих его концах (internal biliari drainag - "double mushroom" a COOK GROUP COMPANY, DK-4632 Bjaeverskov, LOT 941423), однако он громоздок из-за того, что удлинено расстояние между "грибовидными" расширениями, а это в свою очередь способствует миграции дренажа. Кроме этого, дренаж имеет всего один просвет, из-за чего высока вероятность его обтурации пищевыми массами, хлопьями фибрина, кристаллами желчных кислот. To avoid drainage migration from the biliary tract, a device was proposed - drainage with mushroom-shaped extensions at both ends (internal biliari drainag - "double mushroom" a COOK GROUP COMPANY, DK-4632 Bjaeverskov, LOT 941423), but it is cumbersome because , which lengthens the distance between the "mushroom" extensions, and this in turn promotes drainage migration. In addition, the drainage has only one lumen, which is why it is highly likely to obstruct with food masses, fibrin flakes, and bile acid crystals.
Задачей данного изобретения является создание "потерянного" дренажа для формирования билиодигестивного анастомоза, который обеспечивает надежную фиксацию последнего в месте анастомоза и снижает риск его обтурации. The objective of the invention is the creation of "lost" drainage for the formation of biliodigestive anastomosis, which provides reliable fixation of the latter at the site of the anastomosis and reduces the risk of obstruction.
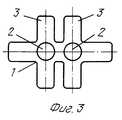
Поставленная задача решается тем, что дренаж состоит из двух одноканальных силиконовых трубок, концы которых выполнены в виде "грибовидных" расширений, причем расстояние между ними составляет 1,5-2 см, что соответствует толщине стенок анастомозируемых органов. The problem is solved in that the drainage consists of two single-channel silicone tubes, the ends of which are made in the form of "mushroom" extensions, and the distance between them is 1.5-2 cm, which corresponds to the wall thickness of the anastomosed organs.
Устройство выполнено с двумя просветами в связи с тем, что при наличии всего одного просвета у дренажа существует большая вероятность обтурации его просвета пищевыми массами, хлопьями фибрина, кристаллами желчных кислот. При наличии трех просветов конструкция становится громоздкой, кроме этого, увеличение просветов или диаметра трубки способствует рефлюксу содержимого желудочно-кишечного тракта в желчные протоки, присоединению холангита. Поэтому суммарный просвет дренажа не должен превышать физиологического просвета холедоха (7-9 мм). The device is made with two lumens due to the fact that if there is only one lumen in the drainage, there is a high probability of obstruction of its lumen with food masses, fibrin flakes, bile acid crystals. In the presence of three gaps, the design becomes cumbersome, in addition, an increase in the gaps or the diameter of the tube contributes to the reflux of the contents of the gastrointestinal tract into the bile ducts, and the attachment of cholangitis. Therefore, the total drainage lumen should not exceed the physiological clearance of the common bile duct (7–9 mm).
Сущность заявленного устройства поясняется чертежом. The essence of the claimed device is illustrated in the drawing.
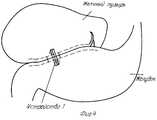
На фиг. 1, 2 представлено продольное сечение дренажа, на фиг.3 - поперечное сечение дренажа, на фиг.4 - стояние дренажа в месте наложенного анастомоза. In FIG. 1, 2 shows a longitudinal section of the drainage, figure 3 is a cross section of the drainage, figure 4 is the standing of the drainage in place of the imposed anastomosis.
Дренаж состоит из двух однопросветных силиковновых трубок 1 и 2. Концы трубок выполнены в виде "грибовидных" расширений 3. Расстояние между "грибовидными" расширениями составляет 1,5-2 см, что соответствует толщине стенок анастомозируемых органов. The drainage consists of two single-
Заявленное устройство работает следующим образом. На стенку желчного пузыря накладывают кисетный шов диаметром, например, 20 мм, в центре которого делают прокол-разрез длинной, например, 5 мм, далее накладывают кисетный шов на стенку желудка, отступая от прокол-разрез, например, 5 мм, диаметром, например, 20 мм, делают прокол-разрез длинной, например, 5 мм внутри кисетного шва. Один конец дренажа 1 с "грибовидным" расширением 3 вводят в просвет желчного пузыря, а другой вводят в просвет желудка, после чего кисетные швы затягивают и завязывают, а между стенками желчного пузыря и желудка накладывают отдельные узловые серозно-серозные швы, в результате чего дренаж оказывается полностью погружен. The claimed device operates as follows. A purse string suture with a diameter of, for example, 20 mm is placed on the wall of the gallbladder, in the center of which a piercing incision is made, for example, 5 mm long, then a purse string suture is made on the stomach wall, departing from a puncture incision, for example, 5 mm, with a diameter, for example , 20 mm, make a puncture incision long, for example, 5 mm inside the purse string suture. One end of
Клинический пример 1. Clinical example 1.
Больная Ш., 66 лет, поступила через 7 суток от начала заболевания. Диагноз: рак поджелудочной железы, осложненный сдавлением дистального отдела холедоха, механической желтухой. Больной проводили консервативную терапию, дообследование, а для устранения гипербилирубинемии выполнили чрескожную чреспеченочную холангиографию, при этом обнаружили опухолевую обтурацию дистального отдела холедоха. Холангиостомический дренаж провести в 12-перстную кишку через обтурацию не удалось, поэтому выполнили наружную гепатикостомию. Однако наружная гепатикостомия ухудшает качество жизни, вызывая дискомфорт в месте стояния дренажа, приводит к потере желчи наружу. Для устранения недостатков наружного дренирования больной выполнили операцию: из "мини"-доступа (длина разреза в правом подреберье составила 6 см) сформировали билиодигестивный анастомоз на разработанном дренаже. Послеоперационный период протекал гладко, больная начала вставать и ходить к концу первых суток после операции. Боли в области послеоперационной раны с 3-го дня прошли. Через 3 суток больной провели контрольное исследование - динамическую холесцинтиографию, на которой пассаж радиофармпрепарата в кишечник в полном объеме без существенной задержки. При контрольных биохимических анализах крови на 3-й день уровень билирубина нормализовался. Больную выписали из стационара на 7-е сутки в удовлетворительном состоянии. Patient Sh., 66 years old, was admitted 7 days after the onset of the disease. Diagnosis: pancreatic cancer, complicated by compression of the distal choledochus, obstructive jaundice. The patient underwent conservative therapy, additional examination, and to eliminate hyperbilirubinemia, percutaneous transhepatic cholangiography was performed, while tumor obstruction of the distal bile duct was found. It was not possible to carry out the cholangiostomy drainage into the duodenum through obstruction, therefore external hepaticostomy was performed. However, external hepaticostomy worsens the quality of life, causing discomfort at the drainage site, leading to the loss of bile outward. To eliminate the shortcomings of external drainage, the patient underwent surgery: from a “mini” approach (the length of the incision in the right hypochondrium was 6 cm), a biliodigestive anastomosis was formed on the developed drainage. The postoperative period was uneventful, the patient began to get up and walk towards the end of the first day after the operation. The pains in the area of the postoperative wound have passed since the 3rd day. After 3 days, the patient conducted a control study - dynamic cholescintiography, in which the passage of the radiopharmaceutical into the intestine in full without significant delay. During control biochemical blood tests on the 3rd day, the bilirubin level returned to normal. The patient was discharged from the hospital on the 7th day in a satisfactory condition.
Таким образом, использование предложенного дренажа для формирования билиодигестивного анастомоза позволяет избежать его миграции и снизить риск обтурации его просвета. Thus, the use of the proposed drainage for the formation of biliodigestive anastomosis avoids its migration and reduces the risk of obstruction of its lumen.
Claims (2)
Translated fromRussianPriority Applications (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| RU2002104566/14ARU2212194C1 (en) | 2002-02-22 | 2002-02-22 | Draining unit for creating biliodigestive anastomosis |
Applications Claiming Priority (1)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| RU2002104566/14ARU2212194C1 (en) | 2002-02-22 | 2002-02-22 | Draining unit for creating biliodigestive anastomosis |
Publications (2)
| Publication Number | Publication Date |
|---|---|
| RU2212194C1true RU2212194C1 (en) | 2003-09-20 |
| RU2002104566A RU2002104566A (en) | 2004-03-20 |
Family
ID=29777451
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| RU2002104566/14ARU2212194C1 (en) | 2002-02-22 | 2002-02-22 | Draining unit for creating biliodigestive anastomosis |
Country Status (1)
| Country | Link |
|---|---|
| RU (1) | RU2212194C1 (en) |
Cited By (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2269365C1 (en)* | 2004-08-20 | 2006-02-10 | Алексей Васильевич Шабунин | Draining tube |
| RU179767U1 (en)* | 2018-01-10 | 2018-05-23 | Янис Ахилесович Чахчахов | Biliary Digestive Shunt |
Citations (3)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US4753236A (en)* | 1986-04-08 | 1988-06-28 | Healey Maureen A | Temporary anastomotic device |
| SU1560134A1 (en)* | 1987-06-01 | 1990-04-30 | С. А. Попов | Device for application of anastomosis |
| SU1595529A1 (en)* | 1987-04-03 | 1990-09-30 | С.А. Попов | Compression probe |
- 2002
- 2002-02-22RURU2002104566/14Apatent/RU2212194C1/ennot_activeIP Right Cessation
Patent Citations (3)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US4753236A (en)* | 1986-04-08 | 1988-06-28 | Healey Maureen A | Temporary anastomotic device |
| SU1595529A1 (en)* | 1987-04-03 | 1990-09-30 | С.А. Попов | Compression probe |
| SU1560134A1 (en)* | 1987-06-01 | 1990-04-30 | С. А. Попов | Device for application of anastomosis |
Cited By (2)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| RU2269365C1 (en)* | 2004-08-20 | 2006-02-10 | Алексей Васильевич Шабунин | Draining tube |
| RU179767U1 (en)* | 2018-01-10 | 2018-05-23 | Янис Ахилесович Чахчахов | Biliary Digestive Shunt |
Also Published As
| Publication number | Publication date |
|---|---|
| RU2002104566A (en) | 2004-03-20 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| RU2212194C1 (en) | Draining unit for creating biliodigestive anastomosis | |
| RU2209601C2 (en) | Method for developing urethralreservoir anastomosis at cystectomy and intestinal plasty of bladder | |
| RU2122361C1 (en) | Method of choledocho- and hepaticojejunostomy | |
| RU2612098C1 (en) | Method for treatment of thoracic esophagus diseases | |
| RU2667873C1 (en) | Method of surgical treatment of high hepatitis choledocha structures in patients with fusion of four lobar hepatic ducts | |
| RU2321355C1 (en) | Method for removing liquor out of cranial cavity in children at hydrocephalus | |
| RU2210327C1 (en) | Method for total substitution of ureter at ileocalicostomy | |
| RU2251984C1 (en) | Method for plasty of perforated gastroduodenal ulcer due to tunnelization | |
| RU2798724C1 (en) | Method of intraoperative prevention of insolvency of the stapler suture line during laparoscopic longitudinal resection of the stomach in patients with obesity and hiatal hernia | |
| RU2804730C1 (en) | Method of forming hepaticojejunostomy | |
| RU2786733C1 (en) | Method for decompression of the bile ducts with clipping of the stump of the cystic duct and fixation to the skin on a teflon conductor | |
| RU2470592C1 (en) | Method of applying antireflux choledochojejunoanastomosis | |
| RU2122360C1 (en) | Method of choledochojejunostomy | |
| RU2674942C1 (en) | Method of treating perforations of the duodenum posterior wall | |
| RU2110961C1 (en) | Method to form large intestinal anastomoses | |
| RU2263517C1 (en) | Method for draining pancreatogastroanastomosis at pancreatoduodenal resection | |
| RU2469655C1 (en) | Method for management of rectal lower ampulla stump | |
| RU2242179C2 (en) | Method for surgical treating cardiac achalasia of iii-iv stages | |
| RU2221502C1 (en) | Method for forming compression-valvular choledochoenteroanastomosis | |
| RU2710215C1 (en) | Method for aseptic organ-preserving resection of hollow organs of the digestive tract | |
| RU2698873C1 (en) | Method of forming hepaticojejunostomy with high bile duct injury | |
| RU2246908C2 (en) | Method for closing perforation gastric openings | |
| SU995752A1 (en) | Method of forming enterostoma | |
| SU1217357A1 (en) | Method of right-hand hemicolectomy | |
| RU2311882C1 (en) | Method for creating pancreaticoenteroanastomosis |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| MM4A | The patent is invalid due to non-payment of fees | Effective date:20050223 |